Lotemax Dailymed
Generic: loteprednol etabonate is used for the treatment of Conjunctivitis, Allergic Conjunctivitis, Bacterial Conjunctivitis, Viral Edema Inflammation Iritis Keratitis Rosacea Eye Infections, Bacterial Eye Infections, Fungal Eye Infections, Viral

Go PRO for all pill images
1 Indications And Usage
LOTEMAX® (loteprednol etabonate ophthalmic ointment) 0.5% ointment is a corticosteroid indicated for the treatment of post-operative inflammation and pain following ocular surgery.
LOTEMAX ointment is a corticosteroid indicated for the treatment of post-operative inflammation and pain following ocular surgery.(1)
2 Dosage And Administration
Wash hands prior to using LOTEMAX ointment.
Apply a small amount (approximately ½ inch ribbon) into the conjunctival sac(s) four times daily beginning 24 hours after surgery and continuing throughout the first 2 weeks of the post-operative period.
Apply a small amount (approximately ½ inch ribbon) into the conjunctival sac(s) four times daily beginning 24 hours after surgery and continuing throughout the first 2 weeks of the post-operative period. (2 )
3 Dosage Forms And Strengths
Ophthalmic ointment containing loteprednol etabonate 0.5%.
Ophthalmic ointment containing loteprednol etabonate 0.5%.(3)
4 Contraindications
LOTEMAX ointment, as with other ophthalmic corticosteroids, is contraindicated in most viral diseases of the cornea and conjunctiva including epithelial herpes simplex keratitis (dendritic keratitis), vaccinia, and varicella, and also in mycobacterial infection of the eye and fungal diseases of ocular structures.
LOTEMAX ointment, as with other ophthalmic corticosteroids, is contraindicated in most viral diseases of the cornea and conjunctiva including epithelial herpes simplex keratitis (dendritic keratitis), vaccinia, and varicella, and also in mycobacterial infection of the eye and fungal diseases of ocular structures. (4 )
5 Warnings And Precautions
• Intraocular Pressure (IOP) Increase: Prolonged use of corticosteroids may result in glaucoma with damage to the optic nerve, defects in visual acuity and fields of vision. If this product is used for 10 days or longer, IOP should be monitored even though it may be difficult in children and uncooperative patients. (5.1 )• Cataracts: Use of corticosteroids may result in posterior subcapsular cataract formation. (5.2 )• Delayed Healing: The use of steroids after cataract surgery may delay healing and increase the incidence of bleb formation. In those diseases causing thinning of the cornea or sclera, perforations have been known to occur with the use of topical steroids. (5.3 )• Bacterial Infections: Prolonged use of corticosteroids may suppress the host response and thus increase the hazard of secondary ocular infections. In acute purulent conditions, steroids may mask infection or enhance existing infection. (5.4 )• Viral Infections: Employment of a corticosteroid medication in the treatment of patients with a history of herpes simplex requires great caution. Use of ocular steroids may prolong the course and may exacerbate the severity of many viral infections of the eye (including herpes simplex). (5.5 )• Fungal Infections: Fungal infections of the cornea are particularly prone to develop coincidentally with long-term local steroid application. Fungus invasion must be considered in any persistent corneal ulceration where a steroid has been used or is in use. (5.6 )5.1 Intraocular Pressure (IOP) Increase
Prolonged use of corticosteroids may result in glaucoma with damage to the optic nerve, defects in visual acuity and fields of vision. Steroids should be used with caution in the presence of glaucoma. If this product is used for 10 days or longer, IOP should be monitored even though it may be difficult in children and uncooperative patients.
5.2 Cataracts
Use of corticosteroids may result in posterior subcapsular cataract formation.
5.3 Delayed Healing
The use of steroids after cataract surgery may delay healing and increase the incidence of bleb formation. In those diseases causing thinning of the cornea or sclera, perforations have been known to occur with the use of topical steroids.
The initial prescription and renewal of the medication order beyond 14 days should be made by a physician only after examination of the patient with the aid of magnification such as slit lamp biomicroscopy and, where appropriate, fluorescein staining.
5.4 Bacterial Infections
Prolonged use of corticosteroids may suppress the host response and thus increase the hazard of secondary ocular infections. In acute purulent conditions, steroids may mask infection or enhance existing infection. If signs and symptoms fail to improve after 2 days, the patient should be re-evaluated.
5.5 Viral Infections
Employment of a corticosteroid medication in the treatment of patients with a history of herpes simplex requires great caution. Use of ocular steroids may prolong the course and may exacerbate the severity of many viral infections of the eye (including herpes simplex).
5.6 Fungal Infections
Fungal infections of the cornea are particularly prone to develop coincidentally with long-term local steroid application. Fungus invasion must be considered in any persistent corneal ulceration where a steroid has been used or is in use. Fungal culture should be taken when appropriate.
5.7 Risk of Contamination
Do not touch the eyelid or surrounding areas with the tip of the tube. The cap should remain on the tube when not in use.
5.8 Contact Lens Wear
Patients should not wear contact lenses during their course of therapy with LOTEMAX ointment.
5.9 Topical Ophthalmic Use
LOTEMAX is not indicated for intraocular administration.
6 Adverse Reactions
Adverse reactions associated with ophthalmic steroids include elevated intraocular pressure, which may be associated with optic nerve damage, visual acuity and field defects, posterior subcapsular cataract formation, secondary ocular infection from pathogens including herpes simplex, and perforation of the globe where there is thinning of the cornea or sclera.
The most common ocular adverse event reported at approximately 25% in subjects in clinical studies with LOTEMAX ointment was anterior chamber inflammation. Other common adverse events, with an incidence of 4-5%, were conjunctival hyperemia, corneal edema, and eye pain. Many of these events may have been the consequence of the surgical procedure. The only non-ocular adverse event occurring at ≥ 1% was headache (1.5%).
The most common ocular adverse event, reported in approximately 25% of subjects in clinical studies, is anterior chamber inflammation. Other common adverse events, with an incidence of 4-5%, are conjunctival hyperemia, corneal edema, and eye pain. (6 )
To report SUSPECTED ADVERSE REACTIONS, contact Bausch & Lomb Incorporated at 1‑800-553-5340 or FDA at 1-800-FDA-1088 orwww.fda.gov/medwatch.
8 Use In Specific Populations
8.1 Pregnancy
Risk Summary
There are no adequate and well-controlled studies with loteprednol etabonate in pregnant women.
Loteprednol etabonate produced teratogenicity at clinically relevant doses in the rabbit and rat when administered orally during pregnancy. Loteprednol etabonate produced malformations when administered orally to pregnant rabbits at doses ≥ 1.6 times the recommended human ophthalmic dose (RHOD) and to pregnant rats at doses ≥ 41 times the RHOD. In pregnant rats receiving oral doses of loteprednol etabonate during the period equivalent to the last trimester of pregnancy through lactation in humans, survival of offspring was reduced at doses ≥ 4 times the RHOD. Maternal toxicity was observed in rats at doses ≥ 405 times the RHOD, and a maternal no observed adverse effect level (NOAEL) was established at 41 times the RHOD.
The background risk of major birth defects and miscarriage for the indicated population is unknown. However, the background risk in the U.S. general population of major birth defects is 2 to 4%, and of miscarriage is 15 to 20%, of clinically recognized pregnancies.
Data
Animal Data
Embryofetal studies were conducted in pregnant rabbits administered loteprednol etabonate by oral gavage on gestation Days 6 to 18, to target the period of organogenesis. Loteprednol etabonate produced fetal malformations at doses ≥ 0.1 mg/kg (1.6 times the recommended human ophthalmic dose (RHOD) based on body surface area, assuming 100% absorption). Spina bifida (including meningocele) was observed at doses ≥ 0.1 mg/kg, and exencephaly and craniofacial malformations were observed at doses ≥ 0.4 mg/kg (6.5 times the RHOD). At 3 mg/kg (49 times the RHOD), loteprednol etabonate was associated with increased incidences of abnormal left common carotid artery, limb flexures, umbilical hernia, scoliosis, and delayed ossification. Abortion and embryofetal lethality (resorption) occurred at doses ≥ 6 mg/kg (97 times the RHOD). A NOAEL for developmental toxicity was not established in this study. The NOAEL for maternal toxicity in rabbits was 3 mg/kg/day.
Embryofetal studies were conducted in pregnant rats administered loteprednol etabonate by oral gavage on gestation Days 6 to 15, to target the period of organogenesis. Loteprednol etabonate produced fetal malformations, including absent innominate artery at doses ≥ 5 mg/kg (41 times the RHOD); and cleft palate, agnathia, cardiovascular defects, umbilical hernia, decreased fetal body weight and decreased skeletal ossification at doses ≥ 50 mg/kg (410 times the RHOD). Embryofetal lethality (resorption) was observed at 100 mg/kg (811 times the RHOD). The NOAEL for developmental toxicity in rats was 0.5 mg/kg (4 times the RHOD). Loteprednol etabonate was maternally toxic (reduced body weight gain) at doses of ≥ 50 mg/kg/day. The NOAEL for maternal toxicity was 5 mg/kg.
A peri-/postnatal study was conducted in rats administered loteprednol etabonate by oral gavage from gestation Day 15 (start of fetal period) to postnatal Day 21 (the end of lactation period). At doses ≥ 0.5 mg/kg (4 times the clinical dose), reduced survival was observed in live-born offspring. Doses ≥ 5 mg/kg (41 times the RHOD) caused umbilical hernia/incomplete gastrointestinal tract. Doses ≥ 50 mg/kg (410 times the RHOD) produced maternal toxicity (reduced body weight gain, death), decreased number of live-born offspring, decreased birth weight, and delays in postnatal development. A developmental NOAEL was not established in this study. The NOAEL for maternal toxicity was 5 mg/kg.
8.2 Lactation
There are no data on the presence of loteprednol etabonate in human milk, the effects on the breastfed infant, or the effects on milk production. The developmental and health benefits of breastfeeding should be considered, along with the mother’s clinical need for LOTEMAX (loteprednol etabonate ophthalmic ointment) 0.5% and any potential adverse effects on the breastfed infant from LOTEMAX.
8.4 Pediatric Use
Safety and effectiveness in pediatric patients have not been established.
8.5 Geriatric Use
No overall differences in safety and effectiveness have been observed between elderly and younger adult patients.
11 Description
LOTEMAX® (loteprednol etabonate ophthalmic ointment) 0.5% is a sterile, topical corticosteroid for ophthalmic use. Loteprednol etabonate is a white to off-white powder.
Loteprednol etabonate is represented by the following structural formula:
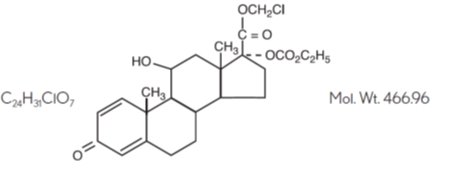
Chemical name:
chloromethyl 17α-[(ethoxycarbonyl)oxy]-11β-hydroxy-3-oxoandrosta-1,4-diene-17β-carboxylate
Each gram contains:
Active: Loteprednol etabonate 5 mg (0.5%);
Inactives: Mineral Oil and White Petrolatum.
12 Clinical Pharmacology
12.1 Mechanism of Action
Corticosteroids inhibit the inflammatory response to a variety of inciting agents and probably delay or slow healing. They inhibit the edema, fibrin deposition, capillary dilation, leukocyte migration, capillary proliferation, fibroblast proliferation, deposition of collagen, and scar formation associated with inflammation. While glucocorticoids are known to bind to and activate the glucocorticoid receptor, the molecular mechanisms involved in glucocorticoid/glucocorticoid receptor‑dependent modulation of inflammation are not clearly established. However, corticosteroids are thought to inhibit prostaglandin production through several independent mechanisms.
12.3 Pharmacokinetics
The systemic exposure to loteprednol etabonate following ocular administration of LOTEMAX ointment has not been studied in humans. However, results from a bioavailability study with LOTEMAX suspension in normal volunteers established that plasma concentrations of loteprednol etabonate and Δ¹ cortienic acid etabonate (PJ 91), its primary, inactive metabolite, were below the limit of quantitation (1 ng/mL) at all sampling times. The results were obtained following the ocular administration of one drop in each eye of 0.5% loteprednol etabonate suspension, 8 times daily for 2 days or 4 times daily for 42 days. The maximum systemic exposure to loteprednol following administration of the ointment product dosed 4 times daily is not expected to exceed exposures attained with LOTEMAX suspension dosed up to two drops 4 times daily.
13 Nonclinical Toxicology
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
Long-term animal studies have not been conducted to evaluate the carcinogenic potential of loteprednol etabonate. Loteprednol etabonate was not genotoxic in vitro in the Ames test, the mouse lymphoma tk assay, or in a chromosome aberration test in human lymphocytes, or in vivo in the single-dose mouse micronucleus assay.
Treatment of female and male rats with doses ≥ 25 mg/kg/day of loteprednol etabonate (203 times the RHOD based on body surface area, assuming 100% absorption) prior to and during mating caused preimplantation loss and decreased the number of live fetuses/live births. The NOAEL for fertility in rats was 5 mg/kg/day (41 times the RHOD).
14 Clinical Studies
In two independent, randomized, multicenter, double-masked, parallel-group, vehicle-controlled studies in 805 subjects meeting a protocol-specified threshold amount of anterior chamber inflammation, LOTEMAX ointment was more effective compared to its vehicle for complete resolution of post-operative anterior chamber cell, flare, and pain following cataract surgery. Primary endpoint was complete resolution of anterior chamber cells and flare (cell count of 0 and no flare) and no pain at post-operative Day 8. The individual clinical trial results are provided below.
In the two studies, LOTEMAX had statistically significant higher incidence of complete clearing of anterior chamber cells and flare at post-operative Day 8 (24-32% vs. 11-14%) and also had a statistically significant higher incidence of subjects that were pain free at post-operative Day 8 (73-78% vs. 41-45%).
16 How Supplied/storage And Handling
LOTEMAX® (loteprednol etabonate ophthalmic ointment) 0.5% is a sterile ointment supplied in a tin tube with a pink polypropylene cap in the following size:
NDC 24208-443-35 3.5 g tube
DO NOT USE IF TAMPER-EVIDENT SKIRT IS VISIBLE ON BOTTOM OF CAP.
Storage: Store between 15°C to 25°C (59°F to 77°F). After opening, LOTEMAX can be used until the expiration date on the tube.
17 Patient Counseling Information
Risk of Contamination
Advise patients to wash hands prior to using LOTEMAX ointment.
Advise patients not to touch the eyelid or surrounding areas with the tip of the tube. The cap should remain on the tube when not in use.
Contact Lens Wear
Advise patients not to wear contact lenses during their course of therapy.
Risk of Secondary Infection
Advise patients to consult a physician if pain, redness, itching or inflammation becomes aggravated [see Warnings and Precautions (5.4)].
Distributed by:
Bausch & Lomb Americas Inc.
Bridgewater, NJ 08807 USA
Manufactured by:
Bausch & Lomb Incorporated
Tampa, FL 33637 USA
LOTEMAX is a trademark of Bausch & Lomb Incorporated or its affiliates.
© 2022 Bausch & Lomb Incorporated or its affiliates
9234905 (Folded)
9234805 (Flat)
Package/label Principal Display Panel
NDC 24208-443-35
BAUSCH + LOMB
Lotemax® loteprednol etabonateophthalmic ointment 0.5%
FOR TOPICAL OPHTHALMIC USE
Rx only
Sterile
Net. Wt. (3.5 g) 1/8oz.
DISCLAIMER:
"This tool does not provide medical advice, and is for informational and educational purposes only, and is not a substitute for professional medical advice, treatment or diagnosis. Call your doctor to receive medical advice. If you think you may have a medical emergency, please dial 911."
"Do not rely on openFDA to make decisions regarding medical care. While we make every effort to ensure that data is accurate, you should assume all results are unvalidated. We may limit or otherwise restrict your access to the API in line with our Terms of Service."
"This product uses publicly available data from the U.S. National Library of Medicine (NLM), National Institutes of Health, Department of Health and Human Services; NLM is not responsible for the product and does not endorse or recommend this or any other product."
PillSync may earn a commission via links on our site
