CellCept (mycophenolate mofetil 500 mg) Dailymed
Generic: mycophenolate mofetil is used for the treatment of Graft vs Host Disease Lactation Psoriasis
IMPRINT: CELLCEPT 250 ROCHE SHAPE: capsule
All Imprints
mycophenolate mofetil 500 mg - roche cellcept 500 cellcept 500 roche oval purple
cellcept (mycophenolate mofetil) tablet, film coated cellcept (mycophenolate mofetil) capsule cellcept (mycophenolate mofetil hydrochloride) injection, powder, lyophilized, for solution cellcept (mycophenolate mofetil) powder, for suspension - roche cellcept 500 oval purple
mycophenolate mofetil 250 mg - cellcept 250 roche capsule
mycophenolate mofetil 500 mg - cellcept 500 roche oval purple
Boxed Warning
Warning: Embryofetal Toxicity, Malignancies And Serious Infections
- Use during pregnancy is associated with increased risks of first trimester pregnancy loss and congenital malformations. Avoid if safer treatment options are available. Females of reproductive potential must be counseled regarding pregnancy prevention and planning [see Warnings and Precautions (5.1), Use in Special Populations (8.1, 8.3)].
- Increased risk of development of lymphoma and other malignancies, particularly of the skin [see Warnings and Precautions (5.2)].
- Increased susceptibility to bacterial, viral, fungal and protozoal infections, including opportunistic infections and viral reactivation of hepatitis B and C, which may lead to hospitalizations and fatal outcomes [see Warnings and Precautions (5.3)].
-
Use during pregnancy is associated with increased risks of first trimester pregnancy loss and congenital malformations. Avoid if safer treatment options are available. Females of reproductive potential must be counseled regarding pregnancy prevention and planning [see
Warnings and Precautions (5.1) ]. -
Increased risk of development of lymphoma and other malignancies, particularly of the skin [see
Warnings and Precautions (5.2) ]. -
Increased susceptibility to infections, including opportunistic infections and severe infections with fatal outcomes [see
Warnings and Precautions (5.3) ].

Go PRO for all pill images
Warning: Embryofetal Toxicity, Malignancies And Serious Infections
- Use during pregnancy is associated with increased risks of first trimester pregnancy loss and congenital malformations. Avoid if safer treatment options are available. Females of reproductive potential must be counseled regarding pregnancy prevention and planning [see Warnings and Precautions (5.1), Use in Special Populations (8.1, 8.3)].
- Increased risk of development of lymphoma and other malignancies, particularly of the skin [see Warnings and Precautions (5.2)].
- Increased susceptibility to bacterial, viral, fungal and protozoal infections, including opportunistic infections and viral reactivation of hepatitis B and C, which may lead to hospitalizations and fatal outcomes [see Warnings and Precautions (5.3)].
WARNING: EMBRYOFETAL TOXICITY, MALIGNANCIES and SERIOUS INFECTIONS
See full prescribing information for complete boxed warning
- Use during pregnancy is associated with increased risks of first trimester pregnancy loss and congenital malformations. Avoid if safer treatment options are available. Females of reproductive potential must be counseled regarding pregnancy prevention and planning [see
Warnings and Precautions (5.1) ].- Increased risk of development of lymphoma and other malignancies, particularly of the skin [see
Warnings and Precautions (5.2) ].- Increased susceptibility to infections, including opportunistic infections and severe infections with fatal outcomes [see
Warnings and Precautions (5.3) ].
Recent Major Changes Section
Indications and Usage, Pediatric Heart or Liver Transplants ( 1 )6/2022 Dosage and Administration, Dosage Recommendations for Heart Transplant Patients ( 2.3 )6/2022 Dosage and Administration, Dosage Recommendations for Liver Transplant Patients ( 2.4 )6/2022 Warnings and Precautions, Serious Infections ( 5.3 )10/2021 Warnings and Precautions, Acute Inflammatory Syndrome Associated with Mycophenolate Products ( 5.7 )10/2021
1 Indications And Usage
CELLCEPT [mycophenolate mofetil (MMF)] is indicated for the prophylaxis of organ rejection, in adult and pediatric recipients 3 months of age and older of allogeneic kidney [see Clinical Studies (14.1)], heart [see Clinical Studies (14.2)] or liver transplants [see Clinical Studies (14.3)], in combination with other immunosuppressants.
CELLCEPT is an antimetabolite immunosuppressant indicated for the prophylaxis of organ rejection in adult and pediatric recipients 3 months of age and older of allogeneic kidney, heart or liver transplants, in combination with other immunosuppressants. (1 )
2 Dosage And Administration
ADULTS DOSAGE Kidney Transplant 1 g twice daily, orally or intravenously (IV) over no less than 2 h ( 2.2 )Heart Transplant 1.5 g twice daily orally or IV, over no less than 2 h ( 2.3 )Liver Transplant 1.5 g twice daily orally or 1g twice daily IV over no less than 2 h ( 2.4 )PEDIATRICS Kidney Transplant 600 mg/m2 orally twice daily, up to maximum of 2 g daily ( 2.2 )Heart Transplant 600 mg/m2 orally twice daily (starting dose) up to a maximum of 900 mg/m2 twice daily (3 g or 15 mL of oral suspension) ( 2.3 )Liver Transplant 600 mg/m2 orally twice daily (starting dose) up to a maximum of 900 mg/m2 twice daily (3 g or 15 mL of oral suspension) ( 2.4 )
- CELLCEPT Intravenous is an alternative when patients cannot tolerate oral medication. Administer within 24 hours following transplantation, until patients can tolerate oral medication, up to 14 days. (
2.1 )- Reduce or interrupt dosing in the event of neutropenia. (
2.5 )- See full prescribing information (FPI) for: adjustments for renal impairment and neutropenia (
2.5 ), preparation of oral suspension and IV solution. (2.6 )2.1 Important Administration Instructions
CELLCEPT should not be used without the supervision of a physician with experience in immunosuppressive therapy.
CELLCEPT Capsules, Tablets and Oral Suspension
CELLCEPT oral dosage forms (capsules, tablets or oral suspension) should not be used interchangeably with mycophenolic acid delayed-release tablets without supervision of a physician with experience in immunosuppressive therapy because the rates of absorption following the administration of CELLCEPT oral dosage forms and mycophenolic acid delayed-release tablets are not equivalent.
CELLCEPT tablets should not be crushed and CELLCEPT capsules should not be opened or crushed. Patients should avoid inhalation or contact of the skin or mucous membranes with the powder contained in CELLCEPT capsules and oral suspension. If such contact occurs, they must wash the area of contact thoroughly with soap and water. In case of ocular contact, rinse eyes with plain water.
The initial oral dose of CELLCEPT should be given as soon as possible following kidney, heart or liver transplant. It is recommended that CELLCEPT be administered on an empty stomach. In stable transplant patients, however, CELLCEPT may be administered with food if necessary [see Clinical Pharmacology (12.3)]. Once reconstituted, CELLCEPT Oral Suspension must not be mixed with any liquids prior to dose administration. If needed, CELLCEPT Oral Suspension can be administered via a nasogastric tube with a minimum size of 8 French (minimum 1.7 mm interior diameter).
Patients should be instructed to take a missed dose as soon as they remember, except if it is closer than 2 hours to the next scheduled dose; in this case, they should continue to take CELLCEPT at the usual times.
CELLCEPT Intravenous
CELLCEPT Intravenous is recommended for patients unable to take oral CELLCEPT. CELLCEPT Intravenous should be administered within 24 hours following transplant. CELLCEPT Intravenous can be administered for up to 14 days; however, patients should be switched to oral CELLCEPT as soon as they can tolerate oral medication.
CELLCEPT Intravenous must be reconstituted before use [see Dosage and Administration (2.6)]. CELLCEPT Intravenous is incompatible with other intravenous infusion solutions and should not be mixed or administered concurrently via the same infusion catheter with other intravenous drugs or infusion admixtures.
CELLCEPT Intravenous must not be administered as a bolus. Following reconstitution, CELLCEPT Intravenous must be administered by slow intravenous infusion over a period of no less than 2 hours by either peripheral or central vein, as rapid infusion increases the risk of local adverse reactions such as phlebitis and thrombosis [see Adverse Reactions (6.1)].
2.2 Dosage Recommendations for Kidney Transplant Patients
Adults
The recommended dosage for adult kidney transplant patients is 1 g orally or intravenously infused over no less than 2 hours, twice daily (total daily dose of 2 g).
Pediatrics (3 months and older)
Pediatric dosing is based on body surface area (BSA). The recommended dosage of CELLCEPT oral suspension for pediatric kidney transplant patients 3 months and older is 600 mg/m2, administered twice daily (maximum total daily dose of 2 g or 10 mL of the oral suspension). Pediatric patients with BSA ‚Č• 1.25 m2 may be dosed with capsules or tablets as follows:
Table 1 Pediatric Kidney Transplant: Dosage Using Capsules or Tablets Body Surface Area Dosage 1.25 m2 to <1.5 m2 CELLCEPT capsule 750 mg twice daily (1.5 g total daily dose) ‚Č• 1.5 m2 CELLCEPT capsules or tablets 1 g twice daily (2 g total daily dose) 2.3 Dosage Recommendations for Heart Transplant Patients
Adults
The recommended dosage of CELLCEPT for adult heart transplant patients is 1.5 g orally or intravenously infused over no less than 2 hours administered twice daily (total daily dose of 3 g).
Pediatrics (3 months and older)
The recommended starting dosage of CELLCEPT oral suspension for pediatric heart transplant patients 3 months and older is 600 mg/m2, administered twice daily. If well tolerated, the dose can be increased to a maintenance dosage of 900 mg/m2 twice daily (maximum total daily dose of 3 g or 15 mL of the oral suspension). The dose may be individualized based on clinical assessment.
Pediatric patients with BSA ‚Č•1.25 m2 may be started on therapy with capsules or tablets as follows:
Table 2 Pediatric Heart Transplant: Pediatric Starting Dosage Using Capsules or Tablets Body Surface Area Starting Dosage Maximum maintenance dose: 3 g total daily. 1.25 m2 to <1.5 m2 CELLCEPT capsule 750 mg twice daily (1.5 g total daily dose) ‚Č• 1.5 m2 CELLCEPT capsules or tablets 1 g twice daily (2 g total daily dose) 2.4 Dosage Recommendations for Liver Transplant Patients
Adults
The recommended dosage of CELLCEPT for adult liver transplant patients is 1.5 g administered orally twice daily (total daily dose of 3 g) or 1 g infused intravenously over no less than 2 hours, twice daily (total daily dose of 2 g).
Pediatrics (3 months and older)
The recommended starting dosage of CELLCEPT oral suspension for pediatric liver transplant patients 3 months of age and older is 600 mg/m2, administered twice daily. If well tolerated, the dose can be increased to a maintenance dosage of 900 mg/m2 twice daily (maximum total daily dose of 3 g or 15 mL of the oral suspension). The dose may be individualized based on clinical assessment.
Pediatric patients with BSA ‚Č•1.25 m2 may be started on therapy with capsules or tablets as follows:
Table 3 Pediatric Liver Transplant: Pediatric Starting Dosage Using Capsules or Tablets Body Surface Area Starting Dosage Maximum maintenance dose: 3 g total daily. 1.25 m2 to <1.5 m2 CELLCEPT capsule 750 mg twice daily (1.5 g total daily dose) ‚Č• 1.5 m2 CELLCEPT capsules or tablets 1 g twice daily (2 g total daily dose) 2.5 Dosage Modifications: Patients with Renal Impairment, Neutropenia
Renal Impairment
No dosage modifications are needed in kidney transplant patients with delayed graft function postoperatively [see Clinical Pharmacology (12.3)]. In kidney transplant patients with severe chronic impairment of the graft (GFR <25 mL/min/1.73 m2), do not administer doses of CELLCEPT greater than 1 g twice a day. These patients should be carefully monitored [see Clinical Pharmacology (12.3)].
Neutropenia
If neutropenia develops (ANC <1.3 √ó 103/¬ĶL), dosing with CELLCEPT should be interrupted or reduced, appropriate diagnostic tests performed, and the patient managed appropriately [see Warnings and Precautions (5.4) and Adverse Reactions (6.1)].
2.6 Preparation Instructions of Oral Suspension and Intravenous for Pharmacists
General Preparation Instructions Before Handling the Formulations
Mycophenolate mofetil (MMF) has demonstrated teratogenic effects in humans. Follow applicable special handling and disposal procedures1 [see Warnings and Precautions (5.1), Adverse Reactions (6.2), Use in Specific Populations (8.1, 8.3), How Supplied/Storage and Handling (16.1)].
Care should be taken to avoid inhalation or direct contact with skin or mucous membranes of the dry powder or the constituted suspension because MMF has demonstrated teratogenic effects in humans. Wearing disposable gloves is recommended during reconstitution and when wiping the outer surface of the bottle/cap and the table surface after reconstitution. If such contact occurs, wash hands thoroughly with soap and water; rinse eyes with water.
Alert patients that they and others should also avoid inhalation or contact of the skin or mucous membranes with the oral suspension. Advise them to wash the area thoroughly with soap and water if such contact occurs; if ocular contact occurs, rinse eyes with plain water.
CELLCEPT Oral Suspension
CELLCEPT Oral Suspension must be reconstituted by the pharmacist prior to dispensing to the patient. CELLCEPT Oral Suspension should not be mixed with any other medication. After reconstitution, the oral suspension contains 200 mg/mL MMF.
Before proceeding with the reconstitution steps read the general preparation instructions above [see General Preparation Instructions Before Handling the Formulations]. The following are the steps for reconstitution:
- Tap the closed bottle several times to loosen the powder.
- Measure 94 mL of water in a graduated cylinder.
- Add approximately half the total amount of water for reconstitution to the bottle and shake the closed bottle well for about 1 minute.
- Add the remainder of water and shake the closed bottle well for about 1 minute.
- Remove the child-resistant cap and push bottle adapter into neck of bottle.
- Close bottle with child-resistant cap tightly. This will assure the proper seating of the bottle adapter in the bottle and child-resistant status of the cap.
- Write the date of expiration of the constituted suspension on the bottle label. (The shelf-life of the constituted suspension is 60 days.)
- Dispense with the "Instruction for Use" and oral dispensers. Alert patients to read the important handling information described in the instructions for use.
Store reconstituted suspension at 25¬įC (77¬įF); excursions permitted to 15¬įC to 30¬įC (59¬įF to 86¬įF). Storage in a refrigerator at 2¬įC to 8¬įC (36¬įF to 46¬įF) is acceptable. Do not freeze. Discard any unused portion 60 days after constitution.
CELLCEPT Intravenous
Before proceeding with the preparation steps for CELLCEPT Intravenous read the general preparation instructions [see General Preparation Instructions Before Handling the Formulations] and note the following:
- CELLCEPT Intravenous does not contain an antibacterial preservative; therefore, reconstitution and dilution of the product must be performed under aseptic conditions.
- This product is sealed under vacuum and should retain a vacuum throughout its shelf life. If a lack of vacuum in the vial is noted while adding the diluent, the vial should not be used.
CELLCEPT Intravenous must be reconstituted and further diluted. A detailed description of the preparation is given below.
Table 4 Preparation Instructions of CELLCEPT Intravenous for Pharmacists Preparation of the 1g dose
- Reconstitute two (2) vials of CELLCEPT Intravenous by injecting 14 mL of 5% Dextrose Injection USP into each vial.
- Gently shake the vial to dissolve the drug.
- Inspect the resulting slightly yellow solution for particulate matter and discoloration prior to further dilution. Discard the vials if particulate matter or discoloration is observed.
- Dilute the contents of the two reconstituted vials (approximately 2 √ó 15 mL) into 140 mL of 5% Dextrose Injection USP.
- Inspect the resulting infusion solution and discard if particulate matter or discoloration is observed.
Preparation of the 1.5 g dose
- Reconstitute three (3) vials of CELLCEPT Intravenous by injecting 14 mL of 5% Dextrose Injection USP into each vial.
- Gently shake the vial to dissolve the drug.
- Inspect the resulting slightly yellow solution for particulate matter and discoloration prior to further dilution. Discard the vials if particulate matter or discoloration is observed.
- Dilute the contents of the three reconstituted vials (approximately 3 √ó 15 mL) into 210 mL of 5% Dextrose Injection USP.
- Inspect the resulting infusion solution and discard if particulate matter or discoloration is observed.
The administration of the infusion should be initiated within 4 hours of reconstitution and dilution of the drug product. Keep solutions at 25¬įC (77¬įF); excursions permitted to 15¬įC to 30¬įC (59¬įF to 86¬įF). Discard unused portion of the reconstituted solutions.
CELLCEPT Injection should not be mixed or administered concurrently via the same infusion catheter with other intravenous drugs or infusion admixtures.
3 Dosage Forms And Strengths
CELLCEPT is available in the following dosage forms and strengths:
Capsules 250 mg mycophenolate mofetil, two-piece hard gelatin capsules, blue-brown, "CELLCEPT 250" printed in black on the blue cap and "Roche" on the brown body Tablets 500 mg mycophenolate mofetil, lavender-colored, caplet-shaped, film-coated tablets engraved with "CELLCEPT 500" on one side and "Roche" on the other For oral suspension 35 g mycophenolate mofetil white to off-white powder for reconstitution (200 mg/mL upon reconstitution) For injection 500 mg mycophenolate mofetil white to off-white lyophilized powder, in a single-dose vial for reconstitution
- Capsules: 250 mg
- Tablets: 500 mg
- For Oral Suspension: 35 g mycophenolate mofetil, powder for reconstitution (200 mg/mL upon reconstitution)
- For Injection: 500 mg mycophenolate mofetil in a single-dose vial for reconstitution.
4 Contraindications
Allergic reactions to CELLCEPT have been observed; therefore, CELLCEPT is contraindicated in patients with a hypersensitivity to mycophenolate mofetil (MMF), mycophenolic acid (MPA) or any component of the drug product. CELLCEPT Intravenous is contraindicated in patients who are allergic to Polysorbate 80 (TWEEN).
- Hypersensitivity to mycophenolate mofetil, mycophenolic acid or any component of the drug product (
4 )- Patients allergic to Polysorbate 80 (present in CELLCEPT IV) (
4 )
5 Warnings And Precautions
- Blood Dyscrasias (Neutropenia, Red Blood Cell Aplasia): Monitor with blood tests; consider treatment interruption or dose reduction. (
5.4 )- Gastrointestinal Complications: Monitor for complications such as bleeding, ulceration and perforations, particularly in patients with underlying gastrointestinal disorders. (
5.5 )- Hypoxanthine-Guanine Phosphoribosyl-Transferase Deficiency: Avoid use of CELLCEPT. (
5.6 )- Acute Inflammatory Syndrome Associated with Mycophenolate Products: Monitor for this paradoxical inflammatory reaction. (
5.7 )- Immunizations: Avoid live attenuated vaccines. (
5.8 )- Local Reactions with Rapid Intravenous Administration: CELLCEPT Intravenous must not be administered by rapid or bolus intravenous injection. (
5.9 )- Phenylketonurics: Oral suspension contains aspartame. (
5.10 )- Blood Donation: Avoid during therapy and for 6 weeks thereafter. (
5.11 )- Semen Donation: Avoid during therapy and for 90 days thereafter. (
5.12 )- Potential Impairment on Driving and Use of Machinery: CELLCEPT may affect ability to drive or operate machinery. (
5.14 )5.1Embryofetal Toxicity
Use of MMF during pregnancy is associated with an increased risk of first trimester pregnancy loss and an increased risk of congenital malformations, especially external ear and other facial abnormalities including cleft lip and palate, and anomalies of the distal limbs, heart, esophagus, kidney and nervous system. Females of reproductive potential must be made aware of these risks and must be counseled regarding pregnancy prevention and planning. Avoid use of MMF during pregnancy if safer treatment options are available [see Use in Specific Populations (8.1, 8.3)].
5.2Lymphoma and Other Malignancies
Patients receiving immunosuppressants, including CELLCEPT, are at increased risk of developing lymphomas and other malignancies, particularly of the skin [see Adverse Reactions (6.1)]. The risk appears to be related to the intensity and duration of immunosuppression rather than to the use of any specific agent. For patients with increased risk for skin cancer, exposure to sunlight and UV light should be limited by wearing protective clothing and using a broad-spectrum sunscreen with a high protection factor.
Post-transplant lymphoproliferative disorder (PTLD) developed in 0.4% to 1% of patients receiving CELLCEPT (2 g or 3 g) with other immunosuppressive agents in controlled clinical trials of kidney, heart and liver transplant patients [see Adverse Reactions (6.1)]. The majority of PTLD cases appear to be related to Epstein Barr Virus (EBV) infection. The risk of PTLD appears greatest in those individuals who are EBV seronegative, a population which includes many young children. In pediatric patients, no other malignancies besides PTLD were observed in clinical trials [see Adverse Reactions (6.1)].
5.3Serious Infections
Patients receiving immunosuppressants, including CELLCEPT, are at increased risk of developing bacterial, fungal, protozoal and new or reactivated viral infections, including opportunistic infections. The risk increases with the total immunosuppressive load. These infections may lead to serious outcomes, including hospitalizations and death [see Adverse Reactions (6.1, 6.2)].
Serious viral infections reported include:
- Polyomavirus-associated nephropathy (PVAN), especially due to BK virus infection
- JC virus-associated progressive multifocal leukoencephalopathy (PML), and
- Cytomegalovirus (CMV) infections: CMV seronegative transplant patients who receive an organ from a CMV seropositive donor are at highest risk of CMV viremia and CMV disease.
- Viral reactivation in patients infected with Hepatitis B and C
COVID-19
Consider dose reduction or discontinuation of CELLCEPT in patients who develop new infections or reactivate viral infections, weighing the risk that reduced immunosuppression represents to the functioning allograft.
PVAN, especially due to BK virus infection, is associated with serious outcomes, including deteriorating renal function and renal graft loss [see Adverse Reactions (6.2)]. Patient monitoring may help detect patients at risk for PVAN.
PML, which is sometimes fatal, commonly presents with hemiparesis, apathy, confusion, cognitive deficiencies, and ataxia [see Adverse Reactions (6.2)]. In immunosuppressed patients, physicians should consider PML in the differential diagnosis in patients reporting neurological symptoms.
The risk of CMV viremia and CMV disease is highest among transplant recipients seronegative for CMV at time of transplant who receive a graft from a CMV seropositive donor. Therapeutic approaches to limiting CMV disease exist and should be routinely provided. Patient monitoring may help detect patients at risk for CMV disease.
Viral reactivation has been reported in patients infected with HBV or HCV. Monitoring infected patients for clinical and laboratory signs of active HBV or HCV infection is recommended.
5.4 Blood Dyscrasias: Neutropenia and Pure Red Cell Aplasia (PRCA)
Severe neutropenia [absolute neutrophil count (ANC) <0.5 √ó 103/¬ĶL] developed in transplant patients receiving CELLCEPT 3 g daily [see Adverse Reactions (6.1)]. Patients receiving CELLCEPT should be monitored for neutropenia. Neutropenia has been observed most frequently in the period from 31 to 180 days post-transplant in patients treated for prevention of kidney, heart and liver rejection. The development of neutropenia may be related to CELLCEPT itself, concomitant medications, viral infections, or a combination of these causes. If neutropenia develops (ANC <1.3 √ó 103/¬ĶL), dosing with CELLCEPT should be interrupted or the dose reduced, appropriate diagnostic tests performed, and the patient managed appropriately [see Dosage and Administration (2.5)].
Patients receiving CELLCEPT should be instructed to report immediately any evidence of infection, unexpected bruising, bleeding or any other manifestation of bone marrow depression.
Consider monitoring with complete blood counts weekly for the first month, twice monthly for the second and third months, and monthly for the remainder of the first year.
Cases of pure red cell aplasia (PRCA) have been reported in patients treated with CELLCEPT in combination with other immunosuppressive agents. In some cases, PRCA was found to be reversible with dose reduction or cessation of CELLCEPT therapy. In transplant patients, however, reduced immunosuppression may place the graft at risk.
5.5 Gastrointestinal Complications
Gastrointestinal bleeding requiring hospitalization, ulceration and perforations were observed in clinical trials. Physicians should be aware of these serious adverse effects particularly when administering CELLCEPT to patients with a gastrointestinal disease.
5.6 Patients with Hypoxanthine-Guanine Phosphoribosyl-Transferase Deficiency (HGPRT)
CELLCEPT is an inosine monophosphate dehydrogenase (IMPDH) inhibitor; therefore it should be avoided in patients with hereditary deficiencies of hypoxanthine-guanine phosphoribosyl-transferase (HGPRT) such as Lesch-Nyhan and Kelley-Seegmiller syndromes because it may cause an exacerbation of disease symptoms characterized by the overproduction and accumulation of uric acid leading to symptoms associated with gout such as acute arthritis, tophi, nephrolithiasis or urolithiasis and renal disease including renal failure.
5.7 Acute Inflammatory Syndrome Associated with Mycophenolate Products
Acute inflammatory syndrome (AIS) has been reported with the use of MMF and mycophenolate products, and some cases have resulted in hospitalization. AIS is a paradoxical pro-inflammatory reaction characterized by fever, arthralgias, arthritis, muscle pain and elevated inflammatory markers including, C-reactive protein and erythrocyte sedimentation rate, without evidence of infection or underlying disease recurrence. Symptoms occur within weeks to months of initiation of treatment or a dose increase. After discontinuation, improvement of symptoms and inflammatory markers are usually observed within 24 to 48 hours.
Monitor patients for symptoms and laboratory parameters of AIS when starting treatment with mycophenolate products or when increasing the dosage. Discontinue treatment and consider other treatment alternatives based on the risk and benefit for the patient.
5.8 Immunizations
During treatment with CELLCEPT, the use of live attenuated vaccines should be avoided (e.g., intranasal influenza, measles, mumps, rubella, oral polio, BCG, yellow fever, varicella, and TY21a typhoid vaccines) and patients should be advised that vaccinations may be less effective. Advise patients to discuss with the physician before seeking any immunizations.
5.9 Local Reactions with Rapid Intravenous Administration
CELLCEPT Intravenous solution must not be administered by rapid or bolus intravenous injection as rapid infusion increases the risk of local adverse reactions such as phlebitis and thrombosis [see Adverse Reactions (6.1)].
5.10 Risks in Patients with Phenylketonuria
Phenylalanine can be harmful to patients with phenylketonuria (PKU). CELLCEPT Oral Suspension contains aspartame, a source of phenylalanine (0.56 mg phenylalanine/mL suspension). Before prescribing CELLCEPT Oral Suspension to a patient with PKU, consider the combined daily amount of phenylalanine from all sources, including CELLCEPT.
5.11 Blood Donation
Patients should not donate blood during therapy and for at least 6 weeks following discontinuation of CELLCEPT because their blood or blood products might be administered to a female of reproductive potential or a pregnant woman.
5.12 Semen Donation
Based on animal data, men should not donate semen during therapy and for 90 days following discontinuation of CELLCEPT [see Use In Specific Populations (8.3)].
5.13 Effect of Concomitant Medications on Mycophenolic Acid Concentrations
A variety of drugs have potential to alter systemic MPA exposure when co-administered with CELLCEPT. Therefore, determination of MPA concentrations in plasma before and after making any changes to immunosuppressive therapy, or when adding or discontinuing concomitant medications, may be appropriate to ensure MPA concentrations remain stable.
5.14 Potential Impairment of Ability to Drive or Operate Machinery
CELLCEPT may impact the ability to drive and use machines. Patients should avoid driving or using machines if they experience somnolence, confusion, dizziness, tremor, or hypotension during treatment with CELLCEPT [see Adverse Reactions (6.1)].
6 Adverse Reactions
The following adverse reactions are discussed in greater detail in other sections of the label:
- Embryofetal Toxicity [see Warnings and Precautions (5.1)]
- Lymphomas and Other Malignancies [see Warnings and Precautions 5.2)]
- Serious Infections [see Warnings and Precautions (5.3)]
- Blood Dyscrasias: Neutropenia, Pure Red Cell Aplasia [see Warnings and Precautions (5.4)]
- Gastrointestinal Complications [see Warnings and Precautions (5.5)]
- Acute Inflammatory Syndrome Associated with Mycophenolate Products [see Warnings and Precautions (5.7)]
The most common adverse reactions in clinical trials (20 % or greater) include diarrhea, leukopenia, infection, vomiting, and there is evidence of a higher frequency of certain types of infections e.g., opportunistic infection. (6.1 )
To report SUSPECTED ADVERSE REACTIONS, contact Genentech at 1-888-835-2555 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.com
6.1 Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
An estimated total of 1557 adult patients received CELLCEPT during pivotal clinical trials in the prevention of acute organ rejection. Of these, 991 were included in the three renal studies, 277 were included in one hepatic study, and 289 were included in one cardiac study. Patients in all study arms also received cyclosporine and corticosteroids.
The data described below primarily derive from five randomized, active-controlled double-blind 12-month trials of CELLCEPT in de novo kidney (3) heart (1) and liver (1) transplant patients [see Clinical Studies (14.1, 14.2, and 14.3)].
CELLCEPT Oral
The incidence of adverse reactions for CELLCEPT was determined in five randomized, comparative, double-blind trials in the prevention of rejection in kidney, heart and liver transplant patients (two active- and one placebo-controlled trials, one active-controlled trial, and one active-controlled trial, respectively) [see Clinical Studies (14.1, 14.2 and 14.3)].
The three de novo kidney studies with 12-month duration compared two dose levels of oral CELLCEPT (1 g twice daily and 1.5 g twice daily) with azathioprine (2 studies) or placebo (1 study) when administered in combination with cyclosporine (Sandimmune¬ģ) and corticosteroids to prevent acute rejection episodes. One study also included anti-thymocyte globulin (ATGAM¬ģ) induction therapy.
In the de novo heart transplantation study with 12-month duration, patients received CELLCEPT 1.5 g twice daily (n=289) or azathioprine 1.5 to 3 mg/kg/day (n=289), in combination with cyclosporine (Sandimmune¬ģ or Neoral¬ģ) and corticosteroids as maintenance immunosuppressive therapy.
In the de novo liver transplantation study with 12-month duration, patients received CELLCEPT 1 g twice daily intravenously for up to 14 days followed by CELLCEPT 1.5 g twice daily orally or azathioprine 1 to 2 mg/kg/day intravenously followed by azathioprine 1 to 2 mg/kg/day orally, in combination with cyclosporine (Neoral¬ģ) and corticosteroids as maintenance immunosuppressive therapy. The total number of patients enrolled was 565.
Approximately 53% of the kidney transplant patients, 65% of the heart transplant patients, and 48% of the liver transplant patients were treated for more than 1 year. Adverse reactions reported in ‚Č• 20% of patients in the CELLCEPT treatment groups are presented below. The safety data of three kidney transplantation studies are pooled together.
Table 5 Adverse Reactions in Controlled Studies of De Novo Kidney, Heart or Liver Transplantation Reported in ‚Č•20% of Patients in the CELLCEPT Group Adverse drug reaction Kidney Studies Heart Study Liver Study CellCept 2g/day (n=501) or 3g/day (n=490) AZA 1 to 2 mg/kg/day or 100 to 150 mg/day Placebo CellCept 3g/day AZA 1.5 to 3 mg/kg/day CellCept 3g/day AZA 1 to 2 mg/kg/day (n=991) (n=326) (n=166) (n=289) (n=289) (n=277) (n=287) System Organ Class % % % % % % % Infections and infestations Bacterial infections 39.9 33.7 37.3 - - 27.4 26.5 Viral infections - "-" Indicates that the incidence was below the cutoff value of 20% for inclusion in the table. - - 31.1 24.9 - - Blood and lymphatic system disorders Anemia 20.0 23.6 2.4 45.0 47.1 43.0 53.0 Ecchymosis - - - 20.1 9.7 - - Leukocytosis - - - 42.6 37.4 22.4 21.3 Leukopenia 28.6 24.8 4.2 34.3 43.3 45.8 39.0 Thrombocytopenia - - - 24.2 28.0 38.3 42.2 Metabolism and nutrition disorders Hypercholesterolemia - - - 46.0 43.9 - - Hyperglycemia - - - 48.4 53.3 43.7 48.8 Hyperkalemia - - - - - 22.0 23.7 Hypocalcemia - - - - - 30.0 30.0 Hypokalemia - - - 32.5 26.3 37.2 41.1 Hypomagnesemia - - - 20.1 14.2 39.0 37.6 Psychiatric disorders Depression - - - 20.1 15.2 - - Insomnia - - - 43.3 39.8 52.3 47.0 Nervous system disorders Dizziness - - - 34.3 33.9 - - Headache - - - 58.5 55.4 53.8 49.1 Tremor - - - 26.3 25.6 33.9 35.5 Cardiac disorders Tachycardia - - - 22.8 21.8 22.0 15.7 Vascular disorders Hypertension 27.5 32.2 19.3 78.9 74.0 62.1 59.6 Hypotension - - - 34.3 40.1 - - Respiratory, thoracic and mediastinal disorders Cough - - - 40.5 32.2 - - Dyspnea - - - 44.3 44.3 31.0 30.3 Pleural effusion - - - - - 34.3 35.9 Gastrointestinal disorders Abdominal pain 22.4 23.0 11.4 41.9 39.4 62.5 51.2 Constipation - - - 43.6 38.8 37.9 38.3 Decreased appetite - - - - - 25.3 17.1 Diarrhea 30.4 20.9 13.9 52.6 39.4 51.3 49.8 Dyspepsia - - - 22.1 22.1 22.4 20.9 Nausea - - - 56.1 60.2 54.5 51.2 Vomiting - - - 39.1 34.6 32.9 33.4 Hepatobiliary disorders Blood lactate dehydrogenase increased - - - 23.5 18.3 - - Hepatic enzyme increased - - - - - 24.9 19.2 Skin and subcutaneous tissues disorders Rash - - - 26.0 20.8 - - Renal and urinary disorders Blood creatinine increased - - - 42.2 39.8 - - Blood urea increased - - - 36.7 34.3 - - General disorders and administration site conditions Asthenia - - - 49.1 41.2 35.4 33.8 Edema "Edema" includes peripheral edema, facial edema, scrotal edema. 21.0 28.2 8.4 67.5 55.7 48.4 47.7 Pain "Pain" includes musculoskeletal pain (myalgia, neck pain, back pain). 24.8 32.2 9.6 79.2 77.5 74.0 77.5 Pyrexia - - - 56.4 53.6 52.3 56.1
In the three de novo kidney studies, patients receiving 2 g/day of CELLCEPT had an overall better safety profile than did patients receiving 3 g/day of CELLCEPT.
Post-transplant lymphoproliferative disease (PTLD, pseudolymphoma) developed in 0.4% to 1% of patients receiving CELLCEPT (2 g or 3 g daily) with other immunosuppressive agents in controlled clinical trials of kidney, heart and liver transplant patients followed for at least 1 year [see Warnings and Precautions (5.2)]. Non-melanoma skin carcinomas occurred in 1.6% to 4.2% of patients, other types of malignancy in 0.7% to 2.1% of patients. Three-year safety data in kidney and heart transplant patients did not reveal any unexpected changes in incidence of malignancy compared to the 1-year data. In pediatric patients, PTLD was observed in 1.35% (2/148) by 12 months post-transplant.
Cytopenias, including leukopenia, anemia, thrombocytopenia and pancytopenia are a known risk associated with mycophenolate and may lead or contribute to the occurrence of infections and hemorrhages [see Warnings and Precautions (5.3)]. Severe neutropenia (ANC <0.5 √ó 103/¬ĶL) developed in up to 2% of kidney transplant patients, up to 2.8% of heart transplant patients and up to 3.6% of liver transplant patients receiving CELLCEPT 3 g daily [see Warnings and Precautions (5.4) and Dosage and Administration (2.5)].
The most common opportunistic infections in patients receiving CELLCEPT with other immunosuppressants were mucocutaneous candida, CMV viremia/syndrome, and herpes simplex. The proportion of patients with CMV viremia/syndrome was 13.5%. In patients receiving CELLCEPT (2 g or 3 g) in controlled studies for prevention of kidney, heart or liver rejection, fatal infection/sepsis occurred in approximately 2% of kidney and heart patients and in 5% of liver patients [see Warnings and Precautions (5.3)].
The most serious gastrointestinal disorders reported were ulceration and hemorrhage, which are known risks associated with CELLCEPT. Mouth, esophageal, gastric, duodenal, and intestinal ulcers often complicated by hemorrhage, as well as hematemesis, melena, and hemorrhagic forms of gastritis and colitis were commonly reported during the pivotal clinical trials, while the most common gastrointestinal disorders were diarrhea, nausea and vomiting. Endoscopic investigation of patients with CELLCEPT-related diarrhea revealed isolated cases of intestinal villous atrophy [see Warnings and Precautions (5.5)].
The following adverse reactions were reported with 3% to <20% incidence in kidney, heart, and liver transplant patients treated with CELLCEPT, in combination with cyclosporine and corticosteroids.
Table 6 Adverse Reactions in Controlled Studies of De Novo Kidney, Heart or Liver Transplantation Reported in 3% to <20% of Patients Treated with CELLCEPT in Combination with Cyclosporine and Corticosteroids System Organ Class Adverse Reactions Body as a Whole cellulitis, chills, hernia, malaise Infections and Infestations fungal infections Hematologic and Lymphatic coagulation disorder, ecchymosis, pancytopenia Urogenital hematuria Cardiovascular hypotension Metabolic and Nutritional acidosis, alkaline phosphatase increased, hyperlipemia, hypophosphatemia, weight loss Digestive esophagitis, flatulence, gastritis, gastrointestinal hemorrhage, hepatitis, ileus, nausea and vomiting, stomach ulcer, stomatitis Neoplasm benign, malignant and unspecified neoplasm Skin and Appendages skin benign neoplasm, skin carcinoma Psychiatric confusional state Nervous hypertonia, paresthesia, somnolence Musculoskeletal arthralgia, myasthenia
Pediatrics
The type and frequency of adverse events in a clinical study for prevention of kidney allograft rejection in 100 pediatric patients 3 months to 18 years of age dosed with CELLCEPT oral suspension 600 mg/m2 twice daily (up to 1 g twice daily) were generally similar to those observed in adult patients dosed with CELLCEPT capsules at a dose of 1 g twice daily with the exception of abdominal pain, fever, infection, pain, sepsis, diarrhea, vomiting, pharyngitis, respiratory tract infection, hypertension, leukopenia, and anemia, which were observed in a higher proportion in pediatric patients.
Safety information in pediatric heart transplant or pediatric liver transplant patients treated with CELLCEPT is supported by an open-label study in pediatric liver transplant patients and publications; the type and frequency of the reported adverse reactions are consistent with those observed in pediatric patients following renal transplant and in adults.
Geriatrics
Geriatric patients (‚Č•65 years), particularly those who are receiving CELLCEPT as part of a combination immunosuppressive regimen, may be at increased risk of certain infections (including cytomegalovirus [CMV] tissue invasive disease) and possibly gastrointestinal hemorrhage and pulmonary edema, compared to younger individuals [see Warnings and Precautions (5.3) and Adverse Reactions (6.1)].
CELLCEPT Intravenous
The safety profile of CELLCEPT Intravenous was determined from a single, double-blind, controlled comparative study of the safety of 2 g/day of intravenous and oral CELLCEPT in kidney transplant patients in the immediate post-transplant period (administered for the first 5 days). The potential venous irritation of CELLCEPT Intravenous was evaluated by comparing the adverse reactions attributable to peripheral venous infusion of CELLCEPT Intravenous with those observed in the intravenous placebo group; patients in the placebo group received active medication by the oral route.
Adverse reactions attributable to peripheral venous infusion were phlebitis and thrombosis, both observed at 4% in patients treated with CELLCEPT Intravenous.
6.2 Postmarketing Experience
The following adverse reactions have been identified during post-approval use of CELLCEPT. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure:
- Embryo-Fetal Toxicity: Congenital malformations and spontaneous abortions, mainly in the first trimester, have been reported following exposure to mycophenolate mofetil (MMF) in combination with other immunosuppressants during pregnancy [see Warnings and Precautions (5.1), and Use in Specific Populations (8.1), (8.3)]. Congenital malformations include:
- Facial malformations: cleft lip, cleft palate, micrognathia, hypertelorism of the orbits- Abnormalities of the ear and eye: abnormally formed or absent external/middle ear, coloboma, microphthalmos- Malformations of the fingers: polydactyly, syndactyly, brachydactyly- Cardiac abnormalities: atrial and ventricular septal defects- Esophageal malformations: esophageal atresia- Nervous system malformations: such as spina bifida.- Cardiovascular: Venous thrombosis has been reported in patients treated with CELLCEPT administered intravenously.
- Digestive: Colitis, pancreatitis
- Hematologic and Lymphatic: Bone marrow failure, cases of pure red cell aplasia (PRCA) and hypogammaglobulinemia have been reported in patients treated with CELLCEPT in combination with other immunosuppressive agents [see Warnings and Precautions (5.4)].
- Immune: Hypersensitivity, hypogammaglobinemia.
- Infections: Meningitis, infectious endocarditis, tuberculosis, atypical mycobacterial infection, progressive multifocal leukoencephalopathy, BK virus infection, viral reactivation of hepatitis B and hepatitis C, protozoal infections [see Warnings and Precautions (5.3)].
- Respiratory: Bronchiectasis, interstitial lung disease, fatal pulmonary fibrosis, have been reported rarely and should be considered in the differential diagnosis of pulmonary symptoms ranging from dyspnea to respiratory failure in post-transplant patients receiving CELLCEPT.
- Vascular: Lymphocele
7 Drug Interactions
- See FPI for drugs that may interfere with systemic exposure and reduce CELLCEPT efficacy: antacids with magnesium or aluminum hydroxide, proton pump inhibitors, drugs that interfere with enterohepatic recirculation, telmisartan, calcium-free phosphate binders. (
7.1 )- CELLCEPT may reduce effectiveness of oral contraceptives. Use of additional barrier contraceptive methods is recommended. (
7.2 )- See FPI for other important drug interactions. (
7 )7.1 Effect of Other Drugs on CELLCEPT
Table 7 Drug Interactions with CELLCEPT that Affect Mycophenolic Acid (MPA) Exposure Antacids with Magnesium or Aluminum Hydroxide Clinical Impact Concomitant use with an antacid containing magnesium or aluminum hydroxide decreases MPA systemic exposure [see Clinical Pharmacology (12.3)], which may reduce CELLCEPT efficacy. Prevention or Management Administer magnesium or aluminum hydroxide containing antacids at least 2h after CELLCEPT administration. Proton Pump Inhibitors (PPIs) Clinical Impact Concomitant use with PPIs decreases MPA systemic exposure [see Clinical Pharmacology (12.3)], which may reduce CELLCEPT efficacy. Prevention or Management Monitor patients for alterations in efficacy when PPIs are co-administered with CELLCEPT. Examples Lansoprazole, pantoprazole Drugs that Interfere with Enterohepatic Recirculation Clinical Impact Concomitant use with drugs that directly interfere with enterohepatic recirculation, or indirectly interfere with enterohepatic recirculation by altering the gastrointestinal flora, can decrease MPA systemic exposure [see Clinical Pharmacology (12.3)], which may reduce CELLCEPT efficacy. Prevention or Management Monitor patients for alterations in efficacy or CELLCEPT related adverse reactions when these drugs are co-administered with CELLCEPT. Examples Cyclosporine A, trimethoprim/sulfamethoxazole, bile acid sequestrants (cholestyramine), rifampin as well as aminoglycoside, cephalosporin, fluoroquinolone and penicillin classes of antimicrobials Drugs Modulating Glucuronidation Clinical Impact Concomitant use with drugs inducing glucuronidation decreases MPA systemic exposure, potentially reducing CELLCEPT efficacy, while use with drugs inhibiting glucuronidation increases MPA systemic exposure [see Clinical Pharmacology (12.3)], which may increase the risk of CELLCEPT related adverse reactions. Prevention or Management Monitor patients for alterations in efficacy or CELLCEPT related adverse reactions when these drugs are co-administered with CELLCEPT. Examples Telmisartan (induces glucuronidation); isavuconazole (inhibits glucuronidation). Calcium Free Phosphate Binders Clinical Impact Concomitant use with calcium free phosphate binders decrease MPA systemic exposure [see Clinical Pharmacology (12.3)], which may reduce CELLCEPT efficacy. Prevention or Management Administer calcium free phosphate binders at least 2 hours after CELLCEPT. Examples Sevelamer 7.2 Effect of CELLCEPT on Other Drugs
Table 8 Drug Interactions with CELLCEPT that Affect Other Drugs Drugs that Undergo Renal Tubular Secretion Clinical Impact When concomitantly used with CELLCEPT, its metabolite MPAG, may compete with drugs eliminated by renal tubular secretion which may increase plasma concentrations and/or adverse reactions associated with these drugs. Prevention or Management Monitor for drug-related adverse reactions in patients with renal impairment. Examples Acyclovir, ganciclovir, probenecid, valacyclovir, valganciclovir Combination Oral Contraceptives Clinical Impact Concomitant use with CELLCEPT decreased the systemic exposure to levonorgestrel, but did not affect the systemic exposure to ethinylestradiol [see Clinical Pharmacology (12.3)], which may result in reduced combination oral contraceptive effectiveness. Prevention or Management Use additional barrier contraceptive methods.
8 Use In Specific Populations
- Male Patients: Sexually active male patients and/or their female partners are recommended to use effective contraception during treatment of the male patient and for at least 90 days after cessation of treatment (
8.3 )8.1 Pregnancy
Pregnancy Exposure Registry
There is a pregnancy exposure registry that monitors pregnancy outcomes in women exposed to mycophenolate during pregnancy and those becoming pregnant within 6 weeks of discontinuing CELLCEPT treatment. To report a pregnancy or obtain information about the registry, visit www.mycophenolateREMS.com or call 1-800-617-8191.
Risk Summary
Use of mycophenolate mofetil (MMF) during pregnancy is associated with an increased risk of first trimester pregnancy loss and an increased risk of multiple congenital malformations in multiple organ systems [see Human Data]. Oral administration of mycophenolate to rats and rabbits during the period of organogenesis produced congenital malformations and pregnancy loss at doses less than the recommended clinical dose (0.01 to 0.05 times the recommended clinical doses in kidney and heart transplant patients) [see Animal Data].
Consider alternative immunosuppressants with less potential for embryofetal toxicity. Risks and benefits of CELLCEPT should be discussed with the pregnant woman.
The estimated background risk of pregnancy loss and congenital malformations in organ transplant populations is not clear. In the U.S. general population, the estimated background risk of major birth defects and miscarriage in clinically recognized pregnancies is 2 to 4% and 15 to 20%, respectively.
Data
Human Data
A spectrum of congenital malformations (including multiple malformations in individual newborns) has been reported in 23 to 27% of live births in MMF exposed pregnancies, based on published data from pregnancy registries. Malformations that have been documented include external ear, eye, and other facial abnormalities including cleft lip and palate, and anomalies of the distal limbs, heart, esophagus, kidney, and nervous system.
Based on published data from pregnancy registries, the risk of first trimester pregnancy loss has been reported at 45 to 49% following MMF exposure.
Animal Data
In animal reproductive toxicology studies, there were increased rates of fetal resorptions and malformations in the absence of maternal toxicity. Oral administration of MMF to pregnant rats from Gestational Day 7 to Day 16 produced increased embryofetal lethality and fetal malformations including anophthalmia, agnathia, and hydrocephaly at doses equivalent to 0.015 and 0.01 times the recommended human doses for renal and cardiac transplant patients, respectively, when corrected for BSA. Oral administration of MMF to pregnant rabbits from Gestational Day 7 to Day 19 produced increased embryofetal lethality and fetal malformations included ectopia cordis, ectopic kidneys, diaphragmatic hernia, and umbilical hernia at dose equivalents as low as 0.05 and 0.03 times the recommended human doses for renal and cardiac transplant patients, respectively, when corrected for BSA.
8.2 Lactation
Risk Summary
There are no data on the presence of mycophenolate in human milk, or the effects on milk production. There are limited data in the National Transplantation Pregnancy Registry on the effects of mycophenolate on a breastfed child [see Data]. Studies in rats treated with MMF have shown mycophenolic acid (MPA) to be present in milk. Because available data are limited, it is not possible to exclude potential risks to a breastfeeding infant.
The developmental and health benefits of breastfeeding should be considered along with the mother's clinical need for CELLCEPT and any potential adverse effects on the breastfed infant from CELLCEPT or from the underlying maternal condition.
Data
Limited information is available from the National Transplantation Pregnancy Registry. Of seven infants reported by the National Transplantation Pregnancy Registry to have been breastfed while the mother was taking mycophenolate, all were born at 34-40 weeks gestation, and breastfed for up to 14 months. No adverse events were reported.
8.3 Females and Males of Reproductive Potential
Females of reproductive potential must be made aware of the increased risk of first trimester pregnancy loss and congenital malformations and must be counseled regarding pregnancy prevention and planning.
Pregnancy Planning
For patients who are considering pregnancy, consider alternative immunosuppressants with less potential for embryofetal toxicity whenever possible. Risks and benefits of CELLCEPT should be discussed with the patient.
Pregnancy Testing
To prevent unplanned exposure during pregnancy, all females of reproductive potential should have a serum or urine pregnancy test with a sensitivity of at least 25 mIU/mL immediately before starting CELLCEPT. Another pregnancy test with the same sensitivity should be done 8 to 10 days later. Repeat pregnancy tests should be performed during routine follow-up visits. Results of all pregnancy tests should be discussed with the patient. In the event of a positive pregnancy test, consider alternative immunosuppressants with less potential for embryofetal toxicity whenever possible.
Contraception
Female Patients
Females of reproductive potential taking CELLCEPT must receive contraceptive counseling and use acceptable contraception (see Table 9 for acceptable contraception methods). Patients must use acceptable birth control during the entire CELLCEPT therapy, and for 6 weeks after stopping CELLCEPT, unless the patient chooses abstinence.
Patients should be aware that CELLCEPT reduces blood levels of the hormones from the oral contraceptive pill and could theoretically reduce its effectiveness [see Drug Interactions (7.2)].
Table 9 Acceptable Contraception Methods for Females of Reproductive Potential Pick from the following birth control options: Option 1 Methods to Use Alone
- Intrauterine devices (IUDs)
- Tubal sterilization
- Patient's partner vasectomy
OR Option 2 Hormone Methods choose 1 Barrier Methods choose 1 Choose One Hormone Method AND One Barrier Method Estrogen and Progesterone Progesterone-only
- Oral Contraceptive Pill
- Transdermal patch
- Vaginal ring
- Injection
- Implant
AND
- Diaphragm with spermicide
- Cervical cap with spermicide
- Contraceptive sponge
- Male condom
- Female condom
OR Option 3 Barrier Methods choose 1 Barrier Methods choose 1 Choose One Barrier Method from each column (must choose two methods)
- Diaphragm with spermicide
- Cervical cap with spermicide
- Contraceptive sponge
AND
- Male condom
- Female condom
Male Patients
Genotoxic effects have been observed in animal studies at exposures exceeding the human therapeutic exposures by approximately 1.25 times. Thus, the risk of genotoxic effects on sperm cells cannot be excluded. Based on this potential risk, sexually active male patients and/or their female partners are recommended to use effective contraception during treatment of the male patient and for at least 90 days after cessation of treatment. Also, based on the potential risk of genotoxic effects, male patients should not donate sperm during treatment with CELLCEPT and for at least 90 days after cessation of treatment [see Use in Special Populations (8.1), Nonclinical Toxicology (13.1), Patient Counseling Information (17.9)].
8.4 Pediatric Use
Safety and effectiveness have been established in pediatric patients 3 months and older for the prophylaxis of organ rejection of allogenic kidney, heart or liver transplants.
Kidney Transplant
Use of CELLCEPT in this population is supported by evidence from adequate and well-controlled studies of CELLCEPT in adults with additional data from one open-label, pharmacokinetic and safety study of CELLCEPT in pediatric patients after receiving allogeneic kidney transplant (100 patients, 3 months to 18 years of age) [see Dosage and Administration (2.2), Adverse Reactions (6.1), Clinical Pharmacology (12.3), Clinical Studies (14.1)].
Heart Transplant and Liver Transplant
Use of CELLCEPT in pediatric heart transplant and liver transplant patients is supported by adequate and well-controlled studies and pharmacokinetic data in adult heart transplant and liver transplant patients. Additional supportive data include pharmacokinetic data in pediatric kidney transplant and pediatric liver transplant patients (8 liver transplant patients, 9 months to 5 years of age, in an open-label, pharmacokinetic and safety study) and published evidence of clinical efficacy and safety in pediatric heart transplant and pediatric liver transplant patients [see Dosage and Administration (2.3, 2.4), Adverse Reactions (6.1), Clinical Pharmacology (12.3), Clinical Studies (14.1)].
8.5 Geriatric Use
Clinical studies of CELLCEPT did not include sufficient numbers of subjects aged 65 and over to determine whether they respond differently from younger subjects. Other reported clinical experience has not identified differences in responses between geriatric and younger patients. In general, dose selection for a geriatric patient should take into consideration the presence of decreased hepatic, renal or cardiac function and of concomitant drug therapies [see Adverse Reactions (6.1), Drug Interactions (7)].
8.6 Patients with Renal Impairment
Patients with Kidney Transplant
No dosage adjustments are needed in kidney transplant patients experiencing delayed graft function postoperatively but patients should be carefully monitored [see Clinical Pharmacology (12.3)]. In kidney transplant patients with severe chronic impairment of the graft (GFR <25 mL/min/1.73 m2), no dose adjustments are necessary; however, doses greater than 1 g administered twice a day should be avoided.
Patients with Heart and Liver Transplant
No data are available for heart or liver transplant patients with severe chronic renal impairment. CELLCEPT may be used for heart or liver transplant patients with severe chronic renal impairment if the potential benefits outweigh the potential risks.
8.7 Patients with Hepatic Impairment
Patients with Kidney Transplant
No dosage adjustments are recommended for kidney transplant patients with severe hepatic parenchymal disease. However, it is not known whether dosage adjustments are needed for hepatic disease with other etiologies [see Clinical Pharmacology (12.3)].
Patients with Heart Transplant
No data are available for heart transplant patients with severe hepatic parenchymal disease.
10 Overdosage
Possible signs and symptoms of acute overdose include hematological abnormalities such as leukopenia and neutropenia, and gastrointestinal symptoms such as abdominal pain, diarrhea, nausea, vomiting, and dyspepsia.
The experience with overdose of CELLCEPT in humans is limited. The reported effects associated with overdose fall within the known safety profile of the drug. The highest dose administered to kidney transplant patients in clinical trials has been 4 g/day. In limited experience with heart and liver transplant patients in clinical trials, the highest doses used were 4 g/day or 5 g/day. At doses of 4 g/day or 5 g/day, there appears to be a higher rate, compared to the use of 3 g/day or less, of gastrointestinal intolerance (nausea, vomiting, and/or diarrhea), and occasional hematologic abnormalities, particularly neutropenia [see Warnings and Precautions (5.4)].
Treatment and Management
MPA and the phenolic glucuronide metabolite of MPA (MPAG) are usually not removed by hemodialysis. However, at high MPAG plasma concentrations (>100 ¬Ķg/mL), small amounts of MPAG are removed. By increasing excretion of the drug, MPA can be removed by bile acid sequestrants, such as cholestyramine [see Clinical Pharmacology (12.3)].
11 Description
CELLCEPT (mycophenolate mofetil) is an antimetabolite immunosuppressant. It is the 2-morpholinoethyl ester of mycophenolic acid (MPA), an immunosuppressive agent; inosine monophosphate dehydrogenase (IMPDH) inhibitor.
The chemical name for mycophenolate mofetil (MMF) is 2-morpholinoethyl (E)-6-(1,3-dihydro-4-hydroxy-6-methoxy-7-methyl-3-oxo-5-isobenzofuranyl)-4-methyl-4-hexenoate. It has an empirical formula of C23H31NO7, a molecular weight of 433.50, and the following structural formula:
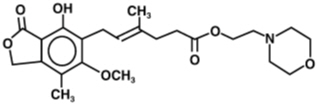
MMF is a white to off-white crystalline powder. It is slightly soluble in water (43 ¬Ķg/mL at pH 7.4); the solubility increases in acidic medium (4.27 mg/mL at pH 3.6). It is freely soluble in acetone, soluble in methanol, and sparingly soluble in ethanol. The apparent partition coefficient in 1-octanol/water (pH 7.4) buffer solution is 238. The pKa values for MMF are 5.6 for the morpholino group and 8.5 for the phenolic group.
MMF hydrochloride has a solubility of 65.8 mg/mL in 5% Dextrose Injection USP (D5W). The pH of the reconstituted solution is 2.4 to 4.1.
CELLCEPT is available for oral administration as capsules containing 250 mg of MMF, tablets containing 500 mg of MMF, and as a powder for oral suspension which, when reconstituted, contains 200 mg/mL of MMF.
Inactive ingredients in CELLCEPT 250 mg capsules include croscarmellose sodium, magnesium stearate, povidone (K-90) and pregelatinized starch. The capsule shells contain black iron oxide, FD&C blue #2, gelatin, red iron oxide, silicon dioxide, sodium lauryl sulfate, titanium dioxide, and yellow iron oxide.
Inactive ingredients in CELLCEPT 500 mg tablets include croscarmellose sodium, magnesium stearate, microcrystalline cellulose, povidone (K-90), and Opadry¬ģ lavender Y-5R-10272-A (hydroxypropyl methylcellulose, hydroxypropyl cellulose, titanium dioxide, polyethylene glycol 400, FD&C Blue No. 2 aluminum lake [indigo carmine aluminum lake], and red iron oxide).
Inactive ingredients in CELLCEPT Oral Suspension include aspartame, citric acid anhydrous, colloidal silicon dioxide, methylparaben, mixed fruit flavor, sodium citrate dihydrate, sorbitol, soybean lecithin, and xanthan gum.
CELLCEPT Intravenous is the hydrochloride salt of MMF. The chemical name for the hydrochloride salt of MMF is 2-morpholinoethyl (E)-6-(1,3-dihydro-4-hydroxy-6-methoxy-7-methyl-3-oxo-5-isobenzofuranyl)-4-methyl-4-hexenoate hydrochloride. It has an empirical formula of C23H31NO7 HCl and a molecular weight of 469.96.
CELLCEPT Intravenous is available as a sterile white to off-white lyophilized powder in single-dose vials containing MMF hydrochloride for administration by intravenous infusion only. Each vial contains 500 mg of mycophenolate mofetil equivalent to 542 mg of mycophenolate mofetil hydrochloride. The inactive ingredients are polysorbate 80, 25 mg, and citric acid, 5 mg. Sodium hydroxide or hydrochloric acid may have been used in the manufacture of CELLCEPT Intravenous to adjust the pH. Reconstitution and dilution with 5% Dextrose Injection USP yields a slightly yellow solution of MMF, 6 mg/mL [see Dosage and Administration (2.6)].
12 Clinical Pharmacology
12.1 Mechanism of Action
Mycophenolate mofetil (MMF) is absorbed following oral administration and hydrolyzed to mycophenolic acid (MPA), the active metabolite. MPA is a selective uncompetitive inhibitor of the two isoforms (type I and type II) of inosine monophosphate dehydrogenase (IMPDH) leading to inhibition of the de novo pathway of guanosine nucleotide synthesis and blocks DNA synthesis. The mechanism of action of MPA is multifaceted and includes effects on cellular checkpoints responsible for metabolic programming of lymphocytes. MPA shifts transcriptional activities in lymphocytes from a proliferative state to catabolic processes. In vitro studies suggest that MPA modulates transcriptional activities in human CD4+ T-lymphocytes by suppressing the Akt/mTOR and STAT5 pathways that are relevant to metabolism and survival, leading to an anergic state of T-cells whereby the cells become less responsive to antigenic stimulation. Additionally, MPA enhanced the expression of negative co-stimulators such as CD70, PD-1, CTLA-4, and transcription factor FoxP3 as well as decreased the expression of positive co-stimulators CD27 and CD28.
MPA decreases proliferative responses of T- and B-lymphocytes to both mitogenic and allo-antigenic stimulation, antibody responses, as well as the production of cytokines from lymphocytes and monocytes such as GM-CSF, IFN-…£, IL-17, and TNF-őĪ. Additionally, MPA prevents the glycosylation of lymphocyte and monocyte glycoproteins that are involved in intercellular adhesion to endothelial cells and may inhibit recruitment of leukocytes into sites of inflammation and graft rejection.
Overall, the effect of MPA is cytostatic and reversible.
12.2 Pharmacodynamics
There is a lack of information regarding the pharmacodynamic effects of MMF.
12.3 Pharmacokinetics
Absorption
Following oral and intravenous administration, MMF undergoes complete conversion to MPA, the active metabolite. In 12 healthy volunteers, the mean absolute bioavailability of oral MMF relative to intravenous MMF was 94%. Two 500 mg CELLCEPT tablets have been shown to be bioequivalent to four 250 mg CELLCEPT capsules. Five mL of the 200 mg/mL constituted CELLCEPT oral suspension have been shown to be bioequivalent to four 250 mg capsules.
The mean (¬ĪSD) pharmacokinetic parameters estimates for MPA following the administration of MMF given as single doses to healthy volunteers, and multiple doses to kidney, heart, and liver transplant patients, are shown in Table 10 . The area under the plasma-concentration time curve (AUC) for MPA appears to increase in a dose-proportional fashion in kidney transplant patients receiving multiple oral doses of MMF up to a daily dose of 3 g (1.5g twice daily) (see Table 10 ).
Table 10 Pharmacokinetic Parameters for MPA [mean (¬ĪSD)] Following Administration of MMF to Healthy Volunteers (Single Dose), and Kidney, Heart, and Liver Transplant Patients (Multiple Doses) Healthy Volunteers Dose/Route Tmax (h) Cmax (mcg/mL) Total AUC(mcg‚ąôh/mL) Single dose 1 g/oral 0.80(¬Ī0.36)(n=129) 24.5(¬Ī9.5)(n=129) 63.9(¬Ī16.2)(n=117) Kidney Transplant Patients (twice daily dosing) Time After Transplantation Dose/Route Tmax (h) Cmax (mcg/mL) Interdosing Interval AUC(0-12h)(mcg‚ąôh/mL) 5 days 1 g/iv 1.58(¬Ī0.46)(n=31) 12.0(¬Ī3.82)(n=31) 40.8(¬Ī11.4)(n=31) 6 days 1 g/oral 1.33(¬Ī1.05)(n=31) 10.7(¬Ī4.83)(n=31) 32.9(¬Ī15.0)(n=31) Early (Less than 40 days) 1 g/oral 1.31(¬Ī0.76)(n=25) 8.16(¬Ī4.50)(n=25) 27.3(¬Ī10.9)(n=25) Early (Less than 40 days) 1.5 g/oral 1.21(¬Ī0.81)(n=27) 13.5(¬Ī8.18)(n=27) 38.4(¬Ī15.4)(n=27) Late (Greater than 3 months) 1.5 g/oral 0.90(¬Ī0.24)(n=23) 24.1(¬Ī12.1)(n=23) 65.3(¬Ī35.4)(n=23) Heart transplant Patients (twice daily dosing) Time After Transplantation Dose/Route Tmax (h) Cmax (mcg/mL) Interdosing Interval AUC(0-12h)(mcg‚ąôh/mL) Early (Day before discharge) 1.5 g/oral 1.8(¬Ī1.3)(n=11) 11.5(¬Ī6.8)(n=11) 43.3(¬Ī20.8)(n=9) Late (Greater than 6 months) 1.5 g/oral 1.1(¬Ī0.7)(n=52) 20.0(¬Ī9.4)(n=52) 54.1 AUC(0-12h) values quoted are extrapolated from data from samples collected over 4 hours. (¬Ī20.4)(n=49)Liver transplant Patients (twice daily dosing) Time After Transplantation Dose/Route Tmax (h) Cmax (mcg/mL) Interdosing Interval AUC(0-12h)(mcg‚ąôh/mL) 4 to 9 days 1 g/iv 1.50(¬Ī0.517)(n=22) 17.0(¬Ī12.7)(n=22) 34.0(¬Ī17.4)(n=22) Early (5 to 8 days) 1.5 g/oral 1.15(¬Ī0.432)(n=20) 13.1(¬Ī6.76)(n=20) 29.2(¬Ī11.9)(n=20) Late (Greater than 6 months) 1.5 g/oral 1.54(¬Ī0.51)(n=6) 19.3(¬Ī11.7)(n=6) 49.3(¬Ī14.8)(n=6)
In the early post-transplant period (less than 40 days post-transplant), kidney, heart, and liver transplant patients had mean MPA AUCs approximately 20% to 41% lower and mean Cmax approximately 32% to 44% lower compared to the late transplant period (i.e., 3 to 6 months post-transplant) (non-stationarity in MPA pharmacokinetics).
Mean MPA AUC values following administration of 1 g twice daily intravenous CELLCEPT over 2 hours to kidney transplant patients for 5 days were about 24% higher than those observed after oral administration of a similar dose in the immediate post-transplant phase.
In liver transplant patients, administration of 1 g twice daily intravenous CELLCEPT followed by 1.5 g twice daily oral CELLCEPT resulted in mean MPA AUC estimates similar to those found in kidney transplant patients administered 1 g CELLCEPT twice daily.
Effect of Food
Food (27 g fat, 650 calories) had no effect on the extent of absorption (MPA AUC) of MMF when administered at doses of 1.5 g twice daily to kidney transplant patients. However, MPA Cmax was decreased by 40% in the presence of food [see Dosage and Administration (2.1)].
Distribution
The mean (¬ĪSD) apparent volume of distribution of MPA in 12 healthy volunteers was approximately 3.6 (¬Ī1.5) L/kg. At clinically relevant concentrations, MPA is 97% bound to plasma albumin. The phenolic glucuronide metabolite of MPA (MPAG) is 82% bound to plasma albumin at MPAG concentration ranges that are normally seen in stable kidney transplant patients; however, at higher MPAG concentrations (observed in patients with kidney impairment or delayed kidney graft function), the binding of MPA may be reduced as a result of competition between MPAG and MPA for protein binding. Mean blood to plasma ratio of radioactivity concentrations was approximately 0.6 indicating that MPA and MPAG do not extensively distribute into the cellular fractions of blood.
In vitro studies to evaluate the effect of other agents on the binding of MPA to human serum albumin (HSA) or plasma proteins showed that salicylate (at 25 mg/dL with human serum albumin) and MPAG (at ‚Č• 460 mcg/mL with plasma proteins) increased the free fraction of MPA. MPA at concentrations as high as 100 mcg/mL had little effect on the binding of warfarin, digoxin or propranolol, but decreased the binding of theophylline from 53% to 45% and phenytoin from 90% to 87%.
Elimination
Mean (¬ĪSD) apparent half-life and plasma clearance of MPA are 17.9 (¬Ī6.5) hours and 193 (¬Ī48) mL/min following oral administration and 16.6 (¬Ī5.8) hours and 177 (¬Ī31) mL/min following intravenous administration, respectively.
Metabolism
The parent drug, MMF, can be measured systemically during the intravenous infusion; however, approximately 5 minutes after the infusion is stopped or after oral administration, MMF concentrations are below the limit of quantitation (0.4 mcg/mL).
Metabolism to MPA occurs pre-systemically after oral dosing. MPA is metabolized principally by glucuronyl transferase to form MPAG, which is not pharmacologically active. In vivo, MPAG is converted to MPA during enterohepatic recirculation. The following metabolites of the 2-hydroxyethyl-morpholino moiety are also recovered in the urine following oral administration of MMF to healthy subjects: N-(2-carboxymethyl)-morpholine, N-(2-hydroxyethyl)-morpholine, and the N-oxide of N-(2-hydroxyethyl)-morpholine.
Due to the enterohepatic recirculation of MPAG/MPA, secondary peaks in the plasma MPA concentration-time profile are usually observed 6 to 12 hours post-dose. Bile sequestrants, such as cholestyramine, reduce MPA AUC by interfering with this enterohepatic recirculation of the drug [see Overdosage (10) and Drug Interaction Studies below].
Excretion
Negligible amount of drug is excreted as MPA (less than 1% of dose) in the urine. Orally administered radiolabeled MMF resulted in complete recovery of the administered dose, with 93% of the administered dose recovered in the urine and 6% recovered in feces. Most (about 87%) of the administered dose is excreted in the urine as MPAG. At clinically encountered concentrations, MPA and MPAG are usually not removed by hemodialysis. However, at high MPAG plasma concentrations (> 100 mcg/mL), small amounts of MPAG are removed.
Increased plasma concentrations of MMF metabolites (MPA 50% increase and MPAG about a 3-fold to 6-fold increase) are observed in patients with renal insufficiency [see Specific Populations].
Specific Populations
Patients with Renal Impairment
The mean (¬ĪSD) pharmacokinetic parameters for MPA following the administration of oral MMF given as single doses to non-transplant subjects with renal impairment are presented in Table 11 .
In a single-dose study, MMF was administered as a capsule or as an intravenous infusion over 40 minutes. Plasma MPA AUC observed after oral dosing to volunteers with severe chronic renal impairment (GFR < 25 mL/min/1.73 m2) was about 75% higher relative to that observed in healthy volunteers (GFR > 80 mL/min/1.73 m2). In addition, the single-dose plasma MPAG AUC was 3-fold to 6-fold higher in volunteers with severe renal impairment than in volunteers with mild renal impairment or healthy volunteers, consistent with the known renal elimination of MPAG. No data are available on the safety of long-term exposure to this level of MPAG.
Plasma MPA AUC observed after single-dose (1 g) intravenous dosing to volunteers (n=4) with severe chronic renal impairment (GFR < 25 mL/min/1.73 m2) was 62.4 mcg‚ąôh/mL (¬Ī19.3). Multiple dosing of MMF in patients with severe chronic renal impairment has not been studied.
Patients with Delayed Graft Function or Nonfunction
In patients with delayed renal graft function post-transplant, mean MPA AUC(0-12h) was comparable to that seen in post-transplant patients without delayed renal graft function. There is a potential for a transient increase in the free fraction and concentration of plasma MPA in patients with delayed renal graft function. However, dose adjustment does not appear to be necessary in patients with delayed renal graft function. Mean plasma MPAG AUC(0-12h) was 2-fold to 3-fold higher than in post-transplant patients without delayed renal graft function [see Dosage and Administration (2.5)].
In eight patients with primary graft non-function following kidney transplantation, plasma concentrations of MPAG accumulated about 6-fold to 8-fold after multiple dosing for 28 days. Accumulation of MPA was about 1-fold to 2-fold.
The pharmacokinetics of MMF are not altered by hemodialysis. Hemodialysis usually does not remove MPA or MPAG. At high concentrations of MPAG (> 100 mcg/mL), hemodialysis removes only small amounts of MPAG.
Patients with Hepatic Impairment
The mean (¬Ī SD) pharmacokinetic parameters for MPA following the administration of oral MMF given as single doses to non-transplant subjects with hepatic impairment is presented in Table 11 .
In a single-dose (1 g oral) study of 18 volunteers with alcoholic cirrhosis and 6 healthy volunteers, hepatic MPA glucuronidation processes appeared to be relatively unaffected by hepatic parenchymal disease when pharmacokinetic parameters of healthy volunteers and alcoholic cirrhosis patients within this study were compared. However, it should be noted that for unexplained reasons, the healthy volunteers in this study had about a 50% lower AUC as compared to healthy volunteers in other studies, thus making comparisons between volunteers with alcoholic cirrhosis and healthy volunteers difficult. In a single-dose (1 g intravenous) study of 6 volunteers with severe hepatic impairment (aminopyrine breath test less than 0.2% of dose) due to alcoholic cirrhosis, MMF was rapidly converted to MPA. MPA AUC was 44.1 mcg‚ąôh/mL (¬Ī15.5).
Table 11 Pharmacokinetic Parameters for MPA [mean (¬ĪSD)] Following Single Doses of MMF Capsules in Chronic Renal and Hepatic Impairment Pharmacokinetic Parameters for Renal Impairment Dose Tmax (h) Cmax (mcg/mL) AUC(0-96h)(mcg‚ąôh/mL) Healthy Volunteers¬†¬†GFR greater than 80 mL/min/1.73 m2 ¬†¬†(n=6) 1 g 0.75(¬Ī0.27) 25.3(¬Ī7.99) 45.0(¬Ī22.6) Mild Renal Impairment¬†¬†GFR 50 to 80 mL/min/1.73 m2 ¬†¬†(n=6) 1 g 0.75(¬Ī0.27) 26.0(¬Ī3.82) 59.9(¬Ī12.9) Moderate Renal Impairment¬†¬†GFR 25 to 49 mL/min/1.73 m2 ¬†¬†(n=6) 1 g 0.75(¬Ī0.27) 19.0(¬Ī13.2) 52.9(¬Ī25.5) Severe Renal Impairment¬†¬†GFR less than 25 mL/min/1.73 m2 ¬†¬†(n=7) 1 g 1.00(¬Ī0.41) 16.3(¬Ī10.8) 78.6(¬Ī46.4) Pharmacokinetic Parameters for Hepatic Impairment Dose Tmax (h) Cmax (mcg/mL) AUC(0-48h)(mcg‚ąôh/mL) Healthy Volunteers¬†¬†(n=6) 1 g 0.63(¬Ī0.14) 24.3(¬Ī5.73) 29.0(¬Ī5.78) Alcoholic Cirrhosis¬†¬†(n=18) 1 g 0.85(¬Ī0.58) 22.4(¬Ī10.1) 29.8(¬Ī10.7)
Pediatric Patients
The pharmacokinetic parameters of MPA and MPAG have been evaluated in 55 pediatric patients (ranging from 1 year to 18 years of age) receiving CELLCEPT oral suspension at a dose of 600 mg/m2 twice daily (up to a maximum of 1 g twice daily) after allogeneic kidney transplantation. The pharmacokinetic data for MPA is provided in Table 12 .
Table 12 Mean (¬ĪSD) Computed Pharmacokinetic Parameters for MPA by Age and Time after Allogeneic Kidney Transplantation Age Group (n) Time Tmax (h) Dose Adjusted adjusted to a dose of 600 mg/m2 Cmax (mcg/mL)Dose Adjusted AUC0-12 (mcg‚ąôh/mL) Early (Day 7) 1 to less than 2 yr (6) a subset of 1 to <6 yr 3.03 (4.70) 10.3 (5.80) 22.5 (6.66) 1 to less than 6 yr (17) 1.63 (2.85) 13.2 (7.16) 27.4 (9.54) 6 to less than 12 yr (16) 0.940 (0.546) 13.1 (6.30) 33.2 (12.1) 12 to 18 yr (21) 1.16 (0.830) 11.7 (10.7) 26.3 (9.14) n=20 Late (Month 3) 1 to less than 2 yr (4) 0.725 (0.276) 23.8 (13.4) 47.4 (14.7) 1 to less than 6 yr (15) 0.989 (0.511) 22.7 (10.1) 49.7 (18.2) 6 to less than 12 yr (14) 1.21 (0.532) 27.8 (14.3) 61.9 (19.6) 12 to 18 yr (17) 0.978 (0.484) 17.9 (9.57) 53.6 (20.3) n=16 Late (Month 9) 1 to less than 2 yr (4) 0.604 (0.208) 25.6 (4.25) 55.8 (11.6) 1 to less than 6 yr (12) 0.869 (0.479) 30.4 (9.16) 61.0 (10.7) 6 to less than 12 yr (11) 1.12 (0.462) 29.2 (12.6) 66.8 (21.2) 12 to 18 yr (14) 1.09 (0.518) 18.1 (7.29) 56.7 (14.0)
The CELLCEPT oral suspension dose of 600 mg/m2 twice daily (up to a maximum of 1 g twice daily) achieved mean MPA AUC values in pediatric patients similar to those seen in adult kidney transplant patients receiving CELLCEPT capsules at a dose of 1 g twice daily in the early post-transplant period. There was wide variability in the data. As observed in adults, early post-transplant MPA AUC values were approximately 45% to 53% lower than those observed in the later post-transplant period (>3 months). MPA AUC values were similar in the early and late post-transplant period across the 1 to 18-year age range.
A comparison of dose-normalized (to 600 mg/m2) MPA AUC values in 12 pediatric kidney transplant patients less than 6 years of age at 9 months post-transplant with those values in 7 pediatric liver transplant patients [median age 17 months (range: 10 ‚Äď 60 months)] and at 6 months and beyond post-transplant revealed that, at the same dose, there were on average 23% lower AUC values in the pediatric liver compared to pediatric kidney patients. This is consistent with the need for higher dosing in adult liver transplant patients compared to kidney transplant patients to achieve the same exposure.
In adult transplant patients administered the same dosage of CELLCEPT, there is similar MPA exposure among kidney transplant and heart transplant patients. Based on the established similarity in MPA exposure between pediatric kidney transplant and adult kidney transplant patients at their respective approved doses, it is expected that MPA exposure at the recommended dosage will be similar in pediatric heart transplant and adult heart transplant patients.
Male and Female Patients
Data obtained from several studies were pooled to look at any gender-related differences in the pharmacokinetics of MPA (data were adjusted to 1 g oral dose). Mean (¬ĪSD) MPA AUC (0-12h) for males (n=79) was 32.0 (¬Ī14.5) and for females (n=41) was 36.5 (¬Ī18.8) mcg‚ąôh/mL while mean (¬ĪSD) MPA Cmax was 9.96 (¬Ī6.19) in the males and 10.6 (¬Ī5.64) mcg/mL in the females. These differences are not of clinical significance.
Geriatric Patients
The pharmacokinetics of mycophenolate mofetil and its metabolites have not been found to be altered in geriatric transplant patients when compared to younger transplant patients.
Drug Interaction Studies
Acyclovir
Coadministration of MMF (1 g) and acyclovir (800 mg) to 12 healthy volunteers resulted in no significant change in MPA AUC and Cmax. However, MPAG and acyclovir plasma AUCs were increased 10.6% and 21.9%, respectively.
Antacids with Magnesium and Aluminum Hydroxides
Absorption of a single dose of MMF (2 g) was decreased when administered to 10 rheumatoid arthritis patients also taking Maalox¬ģ TC (10 mL qid). The Cmax and AUC(0-24h) for MPA were 33% and 17% lower, respectively, than when MMF was administered alone under fasting conditions.
Proton Pump Inhibitors (PPIs)
Coadministration of PPIs (e.g., lansoprazole, pantoprazole) in single doses to healthy volunteers and multiple doses to transplant patients receiving CELLCEPT has been reported to reduce the exposure to MPA. An approximate reduction of 30 to 70% in the Cmax and 25% to 35% in the AUC of MPA has been observed, possibly due to a decrease in MPA solubility at an increased gastric pH.
Cholestyramine
Following single-dose administration of 1.5 g MMF to 12 healthy volunteers pretreated with 4 g three times a day of cholestyramine for 4 days, MPA AUC decreased approximately 40%. This decrease is consistent with interruption of enterohepatic recirculation which may be due to binding of recirculating MPAG with cholestyramine in the intestine.
Cyclosporine
Cyclosporine (Sandimmune¬ģ) pharmacokinetics (at doses of 275 to 415 mg/day) were unaffected by single and multiple doses of 1.5 g twice daily of MMF in 10 stable kidney transplant patients. The mean (¬ĪSD) AUC(0-12h) and Cmax of cyclosporine after 14 days of multiple doses of MMF were 3290 (¬Ī822) ng‚ąôh/mL and 753 (¬Ī161) ng/mL, respectively, compared to 3245 (¬Ī1088) ng‚ąôh/mL and 700 (¬Ī246) ng/mL, respectively, 1 week before administration of MMF.
Cyclosporine A interferes with MPA enterohepatic recirculation. In kidney transplant patients, mean MPA exposure (AUC(0-12h)) was approximately 30-50% greater when MMF was administered without cyclosporine compared with when MMF was coadministered with cyclosporine. This interaction is due to cyclosporine inhibition of multidrug-resistance-associated protein 2 (MRP-2) transporter in the biliary tract, thereby preventing the excretion of MPAG into the bile that would lead to enterohepatic recirculation of MPA. This information should be taken into consideration when MMF is used without cyclosporine.
Drugs Affecting Glucuronidation
Concomitant administration of drugs inhibiting glucuronidation of MPA may increase MPA exposure (e.g., increase of MPA AUC (0-‚ąě) by 35% was observed with concomitant administration of isavuconazole).
Concomitant administration of telmisartan and CELLCEPT resulted in an approximately 30% decrease in MPA concentrations. Telmisartan changes MPA's elimination by enhancing PPAR gamma (peroxisome proliferator-activated receptor gamma) expression, which in turn results in an enhanced UGT1A9 expression and glucuronidation activity.
Ganciclovir
Following single-dose administration to 12 stable kidney transplant patients, no pharmacokinetic interaction was observed between MMF (1.5 g) and intravenous ganciclovir (5 mg/kg). Mean (¬ĪSD) ganciclovir AUC and Cmax (n=10) were 54.3 (¬Ī19.0) mcg‚ąôh/mL and 11.5 (¬Ī1.8) mcg/mL, respectively, after coadministration of the two drugs, compared to 51.0 (¬Ī17.0) mcg‚ąôh/mL and 10.6 (¬Ī2.0) mcg/mL, respectively, after administration of intravenous ganciclovir alone. The mean (¬ĪSD) AUC and Cmax of MPA (n=12) after coadministration were 80.9 (¬Ī21.6) mcg‚ąôh/mL and 27.8 (¬Ī13.9) mcg/mL, respectively, compared to values of 80.3 (¬Ī16.4) ¬Ķg‚ąôh/mL and 30.9 (¬Ī11.2) mcg/mL, respectively, after administration of MMF alone.
Oral Contraceptives
A study of coadministration of CELLCEPT (1 g twice daily) and combined oral contraceptives containing ethinylestradiol (0.02 mg to 0.04 mg) and levonorgestrel (0.05 mg to 0.20 mg), desogestrel (0.15 mg) or gestodene (0.05 mg to 0.10 mg) was conducted in 18 women with psoriasis over 3 consecutive menstrual cycles. Mean serum levels of LH, FSH and progesterone were not significantly affected. Mean AUC(0-24h) was similar for ethinylestradiol and 3-keto desogestrel; however, mean levonorgestrel AUC(0-24h) significantly decreased by about 15%. There was large inter-patient variability (%CV in the range of 60% to 70%) in the data, especially for ethinylestradiol.
Sevelamer
Concomitant administration of sevelamer and MMF in adult and pediatric patients decreased the mean MPA Cmax and AUC (0-12h) by 36% and 26% respectively.
Antimicrobials
Antimicrobials eliminating beta-glucuronidase-producing bacteria in the intestine (e.g. aminoglycoside, cephalosporin, fluoroquinolone, and penicillin classes of antimicrobials) may interfere with the MPAG/MPA enterohepatic recirculation thus leading to reduced systemic MPA exposure. Information concerning antibiotics is as follows:
- Trimethoprim/Sulfamethoxazole: Following single-dose administration of MMF (1.5 g) to 12 healthy male volunteers on day 8 of a 10-day course of trimethoprim 160 mg/sulfamethoxazole 800 mg administered twice daily, no effect on the bioavailability of MPA was observed. The mean (¬ĪSD) AUC and Cmax of MPA after concomitant administration were 75.2 (¬Ī19.8) mcg‚ąôh/mL and 34.0 (¬Ī6.6) ¬Ķg/mL, respectively, compared to 79.2 (¬Ī27.9) mcg‚ąôh/mL and 34.2 (¬Ī10.7) mcg/mL, respectively, after administration of MMF alone.
- Norfloxacin and Metronidazole: Following single-dose administration of MMF (1 g) to 11 healthy volunteers on day 4 of a 5-day course of a combination of norfloxacin and metronidazole, the mean MPA AUC(0-48h) was significantly reduced by 33% compared to the administration of MMF alone (p<0.05). The mean (¬ĪSD) MPA AUC(0-48h) after coadministration of MMF with norfloxacin or metronidazole separately was 48.3 (¬Ī24) mcg‚ąôh/mL and 42.7 (¬Ī23) mcg‚ąôh/mL, respectively, compared with 56.2 (¬Ī24) mcg‚ąôh/mL after administration of MMF alone.
- Ciprofloxacin and Amoxicillin Plus Clavulanic Acid: A total of 64 CELLCEPT-treated kidney transplant recipients received either oral ciprofloxacin 500 mg twice daily or amoxicillin plus clavulanic acid 375 mg three times daily for 7 or at least 14 days, respectively. Approximately 50% reductions in median trough MPA concentrations (pre-dose) from baseline (CELLCEPT alone) were observed in 3 days following commencement of oral ciprofloxacin or amoxicillin plus clavulanic acid. These reductions in trough MPA concentrations tended to diminish within 14 days of antimicrobial therapy and ceased within 3 days of discontinuation of antibiotics.
- Rifampin: In a single heart-lung transplant patient, after correction for dose, a 67% decrease in MPA exposure (AUC(0-12h)) has been observed with concomitant administration of MMF and rifampin.
13 Nonclinical Toxicology
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
In a 104-week oral carcinogenicity study in mice, MMF in daily doses up to 180 mg/kg was not tumorigenic. The highest dose tested was 0.2 times the recommended clinical dose (2 g/day) in renal transplant patients and 0.15 times the recommended clinical dose (3 g/day) in cardiac transplant patients when corrected for differences in body surface area (BSA). In a 104-week oral carcinogenicity study in rats, MMF in daily doses up to 15 mg/kg was not tumorigenic. The highest dose was 0.035 times the recommended clinical dose in kidney transplant patients and 0.025 times the recommended clinical dose in heart transplant patients when corrected for BSA. While these animal doses were lower than those given to patients, they were maximal in those species and were considered adequate to evaluate the potential for human risk [see Warnings and Precautions (5.2)].
The genotoxic potential of MMF was determined in five assays. MMF was genotoxic in the mouse lymphoma/thymidine kinase assay and the in vivo mouse micronucleus assay. MMF was not genotoxic in the bacterial mutation assay, the yeast mitotic gene conversion assay or the Chinese hamster ovary cell chromosomal aberration assay.
MMF had no effect on fertility of male rats at oral doses up to 20 mg/kg/day. This dose represents 0.05 times the recommended clinical dose in renal transplant patients and 0.03 times the recommended clinical dose in cardiac transplant patients when corrected for BSA. In a female fertility and reproduction study conducted in rats, oral doses of 4.5 mg/kg/day caused malformations (principally of the head and eyes) in the first generation offspring in the absence of maternal toxicity. This dose was 0.01 times the recommended clinical dose in renal transplant patients and 0.005 times the recommended clinical dose in cardiac transplant patients when corrected for BSA. No effects on fertility or reproductive parameters were evident in the dams or in the subsequent generation.
14 Clinical Studies
14.1 Kidney Transplantation
Adults
The three de novo kidney transplantation studies compared two dose levels of oral CELLCEPT (1 g twice daily and 1.5 g twice daily) with azathioprine (2 studies) or placebo (1 study) to prevent acute rejection episodes. One of the two studies with azathioprine (AZA) control arm also included anti-thymocyte globulin (ATGAM¬ģ) induction therapy. The geographic location of the investigational sites of these studies are included in Table 13 .
In all three de novo kidney transplantation studies, the primary efficacy endpoint was the proportion of patients in each treatment group who experienced treatment failure within the first 6 months after transplantation. Treatment failure was defined as biopsy-proven acute rejection on treatment or the occurrence of death, graft loss or early termination from the study for any reason without prior biopsy-proven rejection.
CELLCEPT, in combination with corticosteroids and cyclosporine, reduced (statistically significant at 0.05 level) the incidence of treatment failure within the first 6 months following transplantation ( Table 13). Patients who prematurely discontinued treatment were followed for the occurrence of death or graft loss, and the cumulative incidence of graft loss and patient death combined are summarized in Table 14 . Patients who prematurely discontinued treatment were not followed for the occurrence of acute rejection after termination.
Table 13 Treatment Failure in De Novo Kidney Transplantation Studies *Does not include death and graft loss as reason for early termination. USA Study CELLCEPT2 g/day CELLCEPT3 g/day AZA1 to 2 mg/kg/day (N=499 patients) (n=167 patients) (n=166 patients) (n=166 patients) All 3 groups received anti-thymocyte globulin induction, cyclosporine and corticosteroids All treatment failures 31.1% 31.3% 47.6% Early termination without prior acute rejection 9.6% 12.7% 6.0% Biopsy-proven rejection episode on treatment 19.8% 17.5% 38.0% Europe/Canada/Australia Study(N=503 patients) CELLCEPT2 g/day(n=173 patients) CELLCEPT3 g/day(n=164 patients) AZA100 to 150 mg/day(n=166 patients) No induction treatment administered; all 3 groups received cyclosporine and corticosteroids. All treatment failures 38.2% 34.8% 50.0% Early termination without prior acute rejection 13.9% 15.2% 10.2% Biopsy-proven rejection episode on treatment 19.7% 15.9% 35.5% Europe Study CELLCEPT2 g/day CELLCEPT3 g/day Placebo (N=491 patients) (n=165 patients) (n=160 patients) (n=166 patients) No induction treatment administered; all 3 groups received cyclosporine and corticosteroids. All treatment failures 30.3% 38.8% 56.0% Early termination without prior acute rejection 11.5% 22.5% 7.2% Biopsy-proven rejection episode on treatment 17.0% 13.8% 46.4%
No advantage of CELLCEPT at 12 months with respect to graft loss or patient death (combined) was established ( Table 14 ). Numerically, patients receiving CELLCEPT 2 g/day and 3 g/day experienced a better outcome than controls in all three studies; patients receiving CELLCEPT 2 g/day experienced a better outcome than CELLCEPT 3 g/day in two of the three studies. Patients in all treatment groups who terminated treatment early were found to have a poor outcome with respect to graft loss or patient death at 1 year.
Table 14 De Novo Kidney Transplantation Studies Cumulative Incidence of Combined Graft Loss or Patient Death at 12 Months Study CELLCEPT2 g/day CELLCEPT3 g/day Control (AZA or Placebo) USA 8.5% 11.5% 12.2% Europe/Canada/Australia 11.7% 11.0% 13.6% Europe 8.5% 10.0% 11.5%
Pediatrics- De Novo Kidney transplantation PK Study with Long Term Follow-Up
One open-label, safety and pharmacokinetic study of CELLCEPT oral suspension 600 mg/m2 twice daily (up to 1 g twice daily) in combination with cyclosporine and corticosteroids was performed at centers in the United States (9), Europe (5) and Australia (1) in 100 pediatric patients (3 months to 18 years of age) for the prevention of renal allograft rejection. CELLCEPT was well tolerated in pediatric patients [see Adverse Reactions (6.1)], and the pharmacokinetics profile was similar to that seen in adult patients dosed with 1 g twice daily CELLCEPT capsules [see Clinical Pharmacology (12.3)]. The rate of biopsy-proven rejection was similar across the age groups (3 months to <6 years, 6 years to <12 years, 12 years to 18 years). The overall biopsy-proven rejection rate at 6 months was comparable to adults. The combined incidence of graft loss (5%) and patient death (2%) at 12 months post-transplant was similar to that observed in adult kidney transplant patients.
14.2 Heart Transplantation
A double-blind, randomized, comparative, parallel-group, multicenter study in primary de novo heart transplant recipients was performed at centers in the United States (20), in Canada (1), in Europe (5) and in Australia (2). The total number of patients enrolled (ITT population) was 650; 72 never received study drug and 578 received study drug (Safety Population). Patients received CELLCEPT 1.5 g twice daily (n=289) or AZA 1.5 to 3 mg/kg/day (n=289), in combination with cyclosporine (Sandimmune¬ģ or Neoral¬ģ) and corticosteroids as maintenance immunosuppressive therapy. The two primary efficacy endpoints were: (1) the proportion of patients who, after transplantation, had at least one endomyocardial biopsy-proven rejection with hemodynamic compromise, or were re-transplanted or died, within the first 6 months, and (2) the proportion of patients who died or were re-transplanted during the first 12 months following transplantation. Patients who prematurely discontinued treatment were followed for the occurrence of allograft rejection for up to 6 months and for the occurrence of death for 1 year.
The analyses of the endpoints showed:
- Rejection: No difference was established between CELLCEPT and AZA with respect to biopsy-proven rejection with hemodynamic compromise.
- Survival: CELLCEPT was shown to be at least as effective as AZA in preventing death or re-transplantation at 1 year (see Table 15 ).
Table 15 De Novo Heart Transplantation Study Rejection at 6 Months/Death or Re-transplantation at 1 Year All Patients (ITT) Treated Patients AZAN = 323 CELLCEPTN = 327 AZAN = 289 CELLCEPTN = 289 Biopsy-proven rejection with hemodynamic compromise at 6 months Hemodynamic compromise occurred if any of the following criteria were met: pulmonary capillary wedge pressure ‚Č•20 mm or a 25% increase; cardiac index <2.0 L/min/m2 or a 25% decrease; ejection fraction ‚ȧ30%; pulmonary artery oxygen saturation ‚ȧ60% or a 25% decrease; presence of new S3 gallop; fractional shortening was ‚ȧ20% or a 25% decrease; inotropic support required to manage the clinical condition. 121 (38%) 120 (37%) 100 (35%) 92 (32%) Death or re-transplantation at 1 year 49 (15.2%) 42 (12.8%) 33 (11.4%) 18 (6.2%) 14.3 Liver Transplantation
A double-blind, randomized, comparative, parallel-group, multicenter study in primary hepatic transplant recipients was performed at centers in the United States (16), in Canada (2), in Europe (4) and in Australia (1). The total number of patients enrolled was 565. Per protocol, patients received CELLCEPT 1 g twice daily intravenously for up to 14 days followed by CELLCEPT 1.5 g twice daily orally or AZA 1 to 2 mg/kg/day intravenously followed by AZA 1 to 2 mg/kg/day orally, in combination with cyclosporine (Neoral¬ģ) and corticosteroids as maintenance immunosuppressive therapy. The actual median oral dose of AZA on study was 1.5 mg/kg/day (range of 0.3 to 3.8 mg/kg/day) initially and 1.26 mg/kg/day (range of 0.3 to 3.8 mg/kg/day) at 12 months. The two primary endpoints were: (1) the proportion of patients who experienced, in the first 6 months post-transplantation, one or more episodes of biopsy-proven and treated rejection or death or re-transplantation, and (2) the proportion of patients who experienced graft loss (death or re-transplantation) during the first 12 months post-transplantation. Patients who prematurely discontinued treatment were followed for the occurrence of allograft rejection and for the occurrence of graft loss (death or re-transplantation) for 1 year.
In combination with corticosteroids and cyclosporine, CELLCEPT demonstrated a lower rate of acute rejection at 6 months and a similar rate of death or re-transplantation at 1 year compared to AZA ( Table 16 ).
Table 16 De Novo Liver Transplantation Study Rejection at 6 Months/Death or Retransplantation at 1 Year AZAN = 287 CELLCEPTN = 278 Biopsy-proven, treated rejection at 6 months (includes death or re-transplantation) 137 (47.7%) 107 (38.5%) Death or re-transplantation at 1 year 42 (14.6%) 41 (14.7%)
15 References
1. "OSHA Hazardous Drugs." OSHA. http://www.osha.gov/SLTC/hazardousdrugs/index.html
16 How Supplied/storage And Handling
16.1 Handling and Disposal
Mycophenolate mofetil (MMF) has demonstrated teratogenic effects in humans [see Warnings and Precautions (5.1) and Use in Specific Populations (8.1)]. CELLCEPT tablets should not be crushed and CELLCEPT capsules should not be opened or crushed. Wearing disposable gloves is recommended during reconstitution and when wiping the outer surface of the bottle/cap and the table after reconstitution. Avoid inhalation or direct contact with skin or mucous membranes of the powder contained in CELLCEPT capsules, CELLCEPT Oral Suspension (before or after constitution), or CELLCEPT Intravenous (during or after preparation) [see Dosage and Administration (2.6)]. Follow applicable special handling and disposal procedures 1.
16.2CELLCEPT (mycophenolate mofetil capsules) 250 mg
CapsulesBlue-brown, two-piece hard gelatin capsules, printed in black with "CELLCEPT 250" on the blue cap and "Roche" on the brown body. Sizes Bottle of 100 NDC 0004-0259-01 Bottle of 500 NDC 0004-0259-43 StorageStore at 25¬įC (77¬įF); excursions permitted to 15¬įC to 30¬įC (59¬įF to 86¬įF) 16.3 CELLCEPT (mycophenolate mofetil tablets) 500 mg
TabletsLavender-colored, caplet-shaped, film-coated tablets engraved with "CELLCEPT 500" on one side and "Roche" on the other Sizes Bottle of 100 NDC 0004-0260-01 Bottle of 500 NDC 0004-0260-43 Storage and Dispensing Information:
- Store at 25¬įC (77¬įF); excursions permitted to 15¬įC to 30¬įC (59¬įF to 86¬įF).
- Dispense in light-resistant containers, such as the manufacturer's original containers.
16.4 CELLCEPT Oral Suspension (mycophenolate mofetil), for oral suspension
For oral suspension: 35 g mycophenolate mofetil, white to off-white powder blend for constitution to a white to off-white mixed-fruit flavor suspension 225 mL bottle with bottle adapter and 2 oral dispensers NDC 0004-0261-29 Storage
- Store dry powder at 25¬įC (77¬įF); excursions permitted to 15¬įC to 30¬įC (59¬įF to 86¬įF).
- Store constituted suspension at 25¬įC (77¬įF); excursions permitted to 15¬įC to 30¬įC (59¬įF to 86¬įF) for up to 60 days. Storage in a refrigerator at 2¬įC to 8¬įC (36¬įF to 46¬įF) is acceptable. Do not freeze.
16.5 CELLCEPT Intravenous (mycophenolate mofetil for injection)
For injection: 500 mg mycophenolate mofetil in a 20 mL sterile single-dose vial cartons of 4 vials Cartons of 4 single-dose vials NDC 0004-0298-09 Storage
- Store powder and reconstituted infusion solution at 25¬įC (77¬įF); excursions permitted to 15¬įC to 30¬įC (59¬įF to 86¬įF).
17 Patient Counseling Information
Advise the patient to read the FDA-approved patient labeling (Medication Guide and Instructions for Use).
17.1Embryofetal Toxicity
Pregnancy loss and malformations
- Inform females of reproductive potential and pregnant women that use of CELLCEPT during pregnancy is associated with an increased risk of first trimester pregnancy loss and an increased risk of congenital malformations. Advise that they must use an acceptable form of contraception [see Warnings and Precautions (5.1), Use in Specific Populations (8.1, 8.3)].
- Encourage pregnant women to enroll in the Pregnancy Exposure Registry. This registry monitors pregnancy outcomes in women exposed to mycophenolate [see Use in Specific Populations (8.1)].
Contraception
- Discuss pregnancy testing, pregnancy prevention and planning with females of reproductive potential [see Use in Specific Populations (8.3)].
- Females of reproductive potential must use an acceptable form of birth control during the entire CELLCEPT therapy and for 6 weeks after stopping CELLCEPT, unless the patient chooses abstinence. CELLCEPT may reduce effectiveness of oral contraceptives. Use of additional barrier contraceptive methods is recommended [see Use in Specific Populations (8.3)].
- For patients who are considering pregnancy, discuss appropriate alternative immunosuppressants with less potential for embryofetal toxicity. Risks and benefits of CELLCEPT should be discussed with the patient.
- Advise sexually active male patients and/or their partners to use effective contraception during the treatment of the male patient and for at least 90 days after cessation of treatment. This recommendation is based on findings of animal studies [see Use in Specific Populations (8.3), Nonclinical Toxicology (13.1)].
17.2 Development of Lymphoma and Other Malignancies
- Inform patients that they are at increased risk of developing lymphomas and other malignancies, particularly of the skin, due to immunosuppression [see Warnings and Precautions (5.2)].
- Advise patients to limit exposure to sunlight and ultraviolet (UV) light by wearing protective clothing and use of broad-spectrum sunscreen with high protection factor.
17.3 Increased Risk of Serious Infections
Inform patients that they are at increased risk of developing a variety of infections due to immunosuppression. Instruct them to contact their physician if they develop any of the signs and symptoms of infection explained in the Medication Guide [see Warnings and Precautions (5.3)].
17.4 Blood Dyscrasias
Inform patients that they are at increased risk for developing blood adverse effects such as anemia or low white blood cells. Advise patients to immediately contact their healthcare provider if they experience any evidence of infection, unexpected bruising, or bleeding, or any other manifestation of bone marrow suppression [see Warnings and Precautions (5.4)].
17.5 Gastrointestinal Tract Complications
Inform patients that CELLCEPT can cause gastrointestinal tract complications including bleeding, intestinal perforations, and gastric or duodenal ulcers. Advise the patient to contact their healthcare provider if they have symptoms of gastrointestinal bleeding, or sudden onset or persistent abdominal pain [see Warnings and Precautions (5.5)].
17.6Acute Inflammatory Syndrome
Inform patients that acute inflammatory reactions have been reported in some patients who received CELLCEPT. Some reactions were severe, requiring hospitalization. Advise patients to contact their physician if they develop fever, joint stiffness, joint pain or muscle pains [see Warnings and Precautions (5.7)].
17.7Immunizations
Inform patients that CELLCEPT can interfere with the usual response to immunizations. Before seeking vaccines on their own, advise patients to discuss first with their physician [see Warnings and Precautions (5.8)].
17.8Administration Instructions
- Advise patients not to crush CELLCEPT tablets and not to open CELLCEPT capsules.
- Advise patients to avoid inhalation or contact of the skin or mucous membranes with the powder contained in CELLCEPT capsules and with the oral suspension. If such contact occurs, they must wash the area of contact thoroughly with soap and water. In case of ocular contact, rinse eyes with plain water.
- Advise patients to take a missed dose as soon as they remember, except if it is closer than 2 hours to the next scheduled dose; in this case they should continue to take CELLCEPT at the usual times.
17.9 Blood Donation
Advise patients not to donate blood during therapy and for at least 6 weeks following discontinuation of CELLCEPT [see Warnings and Precautions (5.11)].
17.10 Semen Donation
Advise males of childbearing potential not to donate semen during therapy and for 90 days following discontinuation of CELLCEPT [see Warnings and Precautions (5.12)].
17.11 Potential to Impair Driving and Use of Machinery
Advise patients that CELLCEPT can affect the ability to drive or operate machines. Patients should avoid driving or operating machines if they experience somnolence, confusion, dizziness, tremor or hypotension during treatment with CELLCEPT [see Warnings and Precautions (5.14)].
Distributed by:
Genentech USA, Inc. A Member of the Roche Group1 DNA WaySouth San Francisco, CA 94080-4990
Spl Medguide Section
This Medication Guide has been approved by the U.S. Food and Drug Administration. Revised: August 2022 MEDICATION GUIDE CELLCEPT¬ģ [SEL-sept](mycophenolate mofetil capsules)(mycophenolate mofetil tablets) CELLCEPT¬ģ [SEL-sept](mycophenolate mofetil for oral suspension) CELLCEPT¬ģ [SEL-sept](mycophenolate mofetil for injection) Read the Medication Guide that comes with CELLCEPT before you start taking it and each time you refill your prescription. There may be new information. This Medication Guide does not take the place of talking with your doctor about your medical condition or treatment. What is the most important information I should know about CELLCEPT?CELLCEPT can cause serious side effects, including:Increased risk of loss of a pregnancy (miscarriage) and higher risk of birth defects. Females who take CELLCEPT during pregnancy have a higher risk of miscarriage during the first 3 months (first trimester), and a higher risk that their baby will be born with birth defects. Increased risk of getting certain cancers. People who take CELLCEPT have a higher risk of getting lymphoma, and other cancers, especially skin cancer. Tell your doctor if you have:
- If you are a female who can become pregnant, your doctor must talk with you about acceptable birth control methods (contraceptive counseling) to use while taking CELLCEPT. You should have 1 pregnancy test immediately before starting CELLCEPT and another pregnancy test 8 to 10 days later. Pregnancy tests should be repeated during routine follow-up visits with your doctor. Talk to your doctor about the results of all of your pregnancy tests.You must use acceptable birth control during your entire CELLCEPT treatment and for 6 weeks after stopping CELLCEPT, unless at any time you choose to avoid sexual intercourse (abstinence) with a man completely. CELLCEPT decreases blood levels of the hormones in birth control pills that you take by mouth. Birth control pills may not work as well while you take CELLCEPT, and you could become pregnant. If you take birth control pills while using CELLCEPT you must also use another form of birth control. Talk to your doctor about other birth control methods that you can use while taking CELLCEPT.
- If you are a sexually active male whose female partner can become pregnant while you are taking CELLCEPT, use effective contraception during treatment and for at least 90 days after stopping CELLCEPT.
- If you plan to become pregnant, talk with your doctor. Your doctor will decide if other medicines to prevent rejection may be right for you.
- If you become pregnant while taking CELLCEPT, do not stop taking CELLCEPT. Call your doctor right away. You and your doctor may decide that other medicines to prevent rejection may be right for you. You and your doctor should report your pregnancy to the Mycophenolate Pregnancy Registry either:
The purpose of this registry is to gather information about the health of you and your baby.
- By phone at 1-800-617-8191 or
- By visiting the REMS website at: www.mycophenolateREMS.com
- unexplained fever, prolonged tiredness, weight loss or lymph node swelling
- a brown or black skin lesion with uneven borders, or one part of the lesion does not look like the other
- a change in the size and color of a mole
- a new skin lesion or bump
- any other changes to your health
Increased risk of getting serious infections. CELLCEPT weakens the body's immune system and affects your ability to fight infections. Serious infections can happen with CELLCEPT and can lead to hospitalizations and death. These serious infections can include:
- Viral infections. Certain viruses can live in your body and cause active infections when your immune system is weak. Viral infections that can happen with CELLCEPT include:
- Shingles, other herpes infections, and cytomegalovirus (CMV). CMV can cause serious tissue and blood infections.
- BK virus. BK virus can affect how your kidney works and cause your transplanted kidney to fail.
- Hepatitis B and C viruses. Hepatitis viruses can affect how your liver works. Talk to your doctor about how hepatitis viruses may affect you.
- COVID-19
- A brain infection called Progressive Multifocal Leukoencephalopathy (PML). In some patients, CELLCEPT may cause an infection of the brain that may cause death. You are at risk for this brain infection because you have a weakened immune system. Call your doctor right away if you have any of the following symptoms:
- weakness on one side of the body
- you do not care about things you usually care about (apathy)
- you are confused or have problems thinking
- you cannot control your muscles
Call your doctor right away if you have any of the following signs and symptoms of infection:
- Fungal infections. Yeasts and other types of fungal infections can happen with CELLCEPT and can cause serious tissue and blood infections (See "What are the possible side effects of CELLCEPT?").
- temperature of 100.5¬įF or greater
- cold symptoms, such as a runny nose or sore throat
- flu symptoms, such as an upset stomach, stomach pain, vomiting or diarrhea
- earache or headache
- pain during urination
- white patches in the mouth or throat
- unexpected bruising or bleeding
- cuts, scrapes or incisions that are red, warm and oozing pus
See "What are the possible side effects of CELLCEPT?" for information about other serious side effects. What is CELLCEPT?
- CELLCEPT is a prescription medicine to prevent rejection (antirejection medicine) in people who have received a kidney, heart or liver transplant. Rejection is when the body's immune system perceives the new organ as a "foreign" threat and attacks it.
- CELLCEPT is used with other medicines containing cyclosporine and corticosteroids.
Who should not take CELLCEPT?Do not take CELLCEPT if you are allergic to mycophenolate mofetil or any of the ingredients in CELLCEPT. See the end of this Medication Guide for a complete ul of ingredients in CELLCEPT. What should I tell my doctor before taking CELLCEPT?Tell your doctor about all of your medical conditions, including if you: Tell your healthcare provider about all the medicines you take, including prescription and over-the-counter medicines, vitamins and herbal supplements. Some medicines may affect the way CELLCEPT works, and CELLCEPT may affect how some medicines work. Especially tell your doctor if you take:
- have any digestive problems, such as ulcers.
- have Phenylketonuria (PKU). CELLCEPT oral suspension contains aspartame (a source of phenylalanine).
- have Lesch-Nyhan syndrome, Kelley-Seegmiller syndrome, or another rare inherited deficiency hypoxanthine-guanine phosphoribosyl-transferase (HGPRT). You should not take CELLCEPT if you have one of these disorders.
- plan to receive any vaccines. People taking CELLCEPT should not receive live vaccines. Some vaccines may not work as well during treatment with CELLCEPT.
- are pregnant or plan to become pregnant. See "What is the most important information I should know about CELLCEPT?"
- are breastfeeding or plan to breastfeed. It is not known if CELLCEPT passes into breast milk. You and your doctor will decide if you will take CELLCEPT or breastfeed.
Know the medicines you take. Keep a ul of them to show to your doctor or nurse and pharmacist when you get a new medicine. Do not take any new medicine without talking with your doctor.
- birth control pills (oral contraceptives). See "What is the most important information I should know about CELLCEPT?"
- sevelamer (Renagel¬ģ, Renvela‚ĄĘ). These products should be taken at least 2 hours after taking CELLCEPT.
- acyclovir (Zovirax¬ģ), valacyclovir (Valtrex¬ģ), ganciclovir (CYTOVENE¬ģ-IV, Vitrasert¬ģ), valganciclovir (VALCYTE¬ģ).
- rifampin (Rifater¬ģ, Rifamate¬ģ, Rimactane¬ģ, Rifadin¬ģ).
- antacids that contain magnesium and aluminum (CELLCEPT and the antacid should not be taken at the same time).
- proton pump inhibitors (PPIs) (Prevacid¬ģ, Protonix¬ģ).
- sulfamethoxazole/trimethoprim (BACTRIM‚ĄĘ, BACTRIM DS‚ĄĘ).
- norfloxacin (Noroxin¬ģ) and metronidazole (Flagyl¬ģ, Flagyl¬ģ ER, Flagyl¬ģ IV, Metro IV, Helidac¬ģ, Pylera‚ĄĘ).
- ciprofloxacin (Cipro¬ģ, Cipro¬ģ XR, Ciloxan¬ģ, Proquin¬ģ XR) and amoxicillin plus clavulanic acid (Augmentin¬ģ, Augmentin XR‚ĄĘ).
- azathioprine (Azasan¬ģ, Imuran¬ģ).
- cholestyramine (Questran Light¬ģ, Questran¬ģ, Locholest Light, Locholest, Prevalite¬ģ).
How should I take CELLCEPT?
- Take CELLCEPT exactly as prescribed.
- Do not stop taking CELLCEPT or change the dose unless your doctor tells you to.
- If you miss a dose of CELLCEPT, or you are not sure when you took your last dose, take your prescribed dose of CELLCEPT as soon as you remember. If your next dose is less than 2 hours away, skip the missed dose and take your next dose at your normal scheduled time. Do not take 2 doses at the same time. Call your doctor if you are not sure what to do.
- Take CELLCEPT capsules, tablets and oral suspension on an empty stomach, unless your doctor tells you otherwise. Do not crush CELLCEPT tablets.
- Do not open or crush CELLCEPT capsules.
- If you are not able to swallow CELLCEPT tablets or capsules, your doctor may prescribe CELLCEPT Oral Suspension. This is a liquid form of CELLCEPT. Your pharmacist will mix the medicine before you pick it up from a pharmacy.
- Do not mix CELLCEPT Oral Suspension with any other medicine. CELLCEPT Oral Suspension should not be mixed with any type of liquids before taking the dose. See the Instructions for Use at the end of this Medication Guide for detailed instructions about how to take CELLCEPT Oral Suspension the right way.
- Do not breathe in (inhale) or let CELLCEPT powder or oral suspension come in contact with your skin or mucous membranes.
- If you accidentally get the powder or oral suspension on the skin, wash the area well with soap and water.
- If you accidentally get the powder or oral suspension in your eyes or other mucous membranes, flush with plain water.
- If you take too much CELLCEPT, call your doctor or the poison control center right away.
What should I avoid while taking CELLCEPT?
- Avoid becoming pregnant. (See "What is the most important information I should know about CELLCEPT?").
- Limit the amount of time you spend in sunlight. Avoid using tanning beds or sunlamps. People who take CELLCEPT have a higher risk of getting skin cancer (See "What is the most important information I should know about CELLCEPT?"). Wear protective clothing when you are in the sun and use a broad-spectrum sunscreen with a high protection factor. This is especially important if your skin is very fair or if you have a family history of skin cancer.
- You should not donate blood while taking CELLCEPT and for at least 6 weeks after stopping CELLCEPT.
- You should not donate sperm while taking CELLCEPT and for 90 days after stopping CELLCEPT.
- CELLCEPT may influence your ability to drive and use machines (See " What are the possible side effects of CELLCEPT? ". If you experience drowsiness, confusion, dizziness, tremor, or low blood pressure during treatment with CELLCEPT, you should be cautious about driving or using heavy machines.
What are the possible side effects of CELLCEPT?CELLCEPT may cause serious side effects, including: The most common side effects of CELLCEPT include:
- See "What is the most important information I should know about CELLCEPT?"
- Low blood cell counts. People taking high doses of CELLCEPT each day may have a decrease in blood counts, including:
Your doctor will do blood tests before you start taking CELLCEPT and during treatment with CELLCEPT to check your blood cell counts. Tell your doctor right away if you have any signs of infection (See "What is the most important information I should know about CELLCEPT?"), including any unexpected bruising or bleeding. Also, tell your doctor if you have unusual tiredness, lack of energy, dizziness or fainting.
- white blood cells, especially neutrophils. Neutrophils fight against bacterial infections. You have a higher chance of getting an infection when your white blood cell count is low. This is most common from 1 month to 6 months after your transplant.
- red blood cells. Red blood cells carry oxygen to your body tissues. You have a higher chance of getting severe anemia when your red blood cell count is low.
- platelets. Platelets help with blood clotting.
- Stomach problems. Stomach problems including intestinal bleeding, a tear in your intestinal wall (perforation) or stomach ulcers can happen in people who take CELLCEPT. Bleeding can be severe and you may have to be hospitalized for treatment. Call your doctor right away if you have sudden or severe stomach-area pain or stomach-area pain that does not go away, or if you have diarrhea.
- Inflammatory reactions. Some people taking CELLCEPT may have an inflammatory reaction with fever, joint stiffness, joint pain, and muscle pain. Some of these reactions may require hospitalization. This reaction could happen within weeks to months after your treatment with CELLCEPT starts or if your dose is increased. Call your doctor right away if you experience these symptoms.
- diarrhea
- blood problems including low white and red blood cell counts
- infections
- blood pressure problems
- fast heartbeat
- swelling of the lower legs, ankles and feet
- changes in laboratory blood levels, including high levels of blood sugar (hyperglycemia)
- stomach problems including diarrhea, constipation, nausea and vomiting
- rash
- nervous system problems such as headache, dizziness and tremor
Side effects that can happen more often in children than in adults taking CELLCEPT include:
- stomach area pain
- fever
- infection
- pain
- blood infection (sepsis)
- diarrhea
- vomiting
- sore throat
- colds (respiratory tract infections)
- high blood pressure
- low white blood cell count
- low red blood cell count
These are not all of the possible side effects of CELLCEPT. Tell your doctor about any side effect that bothers you or that does not go away. Call your doctor for medical advice about side effects. You may report side effects to FDA at 1-800-FDA-1088.You may also report side effects to Genentech at 1-888-835-2555. How should I store CELLCEPT? Keep CELLCEPT and all medicines out of the reach of children.
- Store CELLCEPT capsules and tablets at room temperature between 59¬įF to 86¬įF (15¬įC to 30¬įC).
- Keep CELLCEPT tablets in the light resistant container that it comes in.
- Store CELLCEPT Oral Suspension at room temperature between 59¬įF to 86¬įF (15¬įC to 30¬įC), for up to 60 days. You can also store CELLCEPT Oral Suspension in the refrigerator between 36¬įF to 46¬įF (2¬įC to 8¬įC). Do not freeze.
General information about the safe and effective use of CELLCEPT. Medicines are sometimes prescribed for purposes other than those uled in a Medication Guide. Do not use CELLCEPT for a condition for which it was not prescribed. Do not give CELLCEPT to other people, even if they have the same symptoms that you have. It may harm them.This Medication Guide summarizes the most important information about CELLCEPT. If you would like more information, talk with your doctor. You can ask your doctor or pharmacist about CELLCEPT that is written for health professionals. What are the ingredients in CELLCEPT?Active ingredient: mycophenolate mofetil Inactive ingredients: CELLCEPT 250 mg capsules: croscarmellose sodium, magnesium stearate, povidone (K-90) and pregelatinized starch. The capsule shells contain black iron oxide, FD&C blue #2, gelatin, red iron oxide, silicon dioxide, sodium lauryl sulfate, titanium dioxide, and yellow iron oxide. CELLCEPT 500 mg tablets: croscarmellose sodium, FD&C blue #2 aluminum lake, hydroxypropyl cellulose, hydroxypropyl methylcellulose, magnesium stearate, microcrystalline cellulose, polyethylene glycol 400, povidone (K-90), red iron oxide, and titanium dioxide. CELLCEPT Oral Suspension: aspartame, citric acid anhydrous, colloidal silicon dioxide, methylparaben, mixed fruit flavor, sodium citrate dihydrate, sorbitol, soybean lecithin, and xanthan gum. CELLCEPT Intravenous: polysorbate 80, and citric acid. Sodium hydroxide and hydrochloric acid may have been used in the manufacture of CELLCEPT Intravenous to adjust the pH. Distributed by: Genentech USA, Inc.A Member of the Roche Group1 DNA WaySouth San Francisco, CA 94080-4990CELLCEPT and VALCYTE are registered trademarks of Hoffmann-La Roche Inc. © 2022 Genentech, Inc. All rights reserved.For more information, call 1-888-835-2555 or visit www.gene.com/gene/products/information/CELLCEPT.
Instructions For Usecellcept [sel-sept](mycophenolate Mofetil) Oral Suspension
Read this Instructions for Use before you take or give CELLCEPT for the first time and each time you get a refill. There may be new information. This information does not take the place of talking to your healthcare provider about your medical condition or treatment.
Important:
- Always use the oral dispenser provided with CELLCEPT Oral Suspension to make sure you measure the right amount of medicine. If your CELLCEPT Oral Suspension does not come with the oral dispenser, contact your pharmacist.
- Call your pharmacist if your oral dispenser is lost or damaged.
- Your pharmacist will write the expiration date on your CELLCEPT Oral Suspension bottle label. Do not use CELLCEPT after the expiration date.
- Ask your doctor or pharmacist if you have any questions or are unsure about how to take or give the right amount of medicine.
- The CELLCEPT Oral Suspension should not be mixed with any type of liquids before taking or giving the dose.
- Do not let the CELLCEPT Oral Suspension come in contact with the skin. If this happens, wash the skin well with soap and water. If the CELLCEPT Oral Suspension gets in the eyes, rinse the eyes with plain water.
- If you spill any CELLCEPT Oral Suspension, wipe it up using paper towels wet with water. Put the child-resistant bottle cap back on the bottle and wipe the outside of the bottle with wet paper towels.
Supplies needed to take or give a dose of CELLCEPT Oral Suspension:
To take or give a dose of CELLCEPT Oral Suspension, you will need the bottle of medicine and the oral dispenser provided with the medicine (See Figure 1 ). Your pharmacist will insert the bottle adapter in the CELLCEPT Oral Suspension bottle. Do not remove the bottle adapter from the bottle.
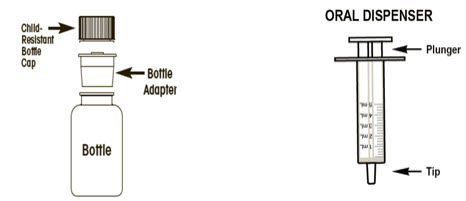
Figure 1
Taking or giving a dose of CELLCEPT Oral Suspension:
Step 1: With the child-resistant cap on the bottle, shake the bottle well for about 5 seconds before each use. Step 2: Open the bottle by firmly pressing down on the child-resistant bottle cap and turning it to the left (counter-clockwise). Do not throw away the child-resistant bottle cap. Step 3: Place the bottle on a flat surface. Before inserting the tip of the oral dispenser into the bottle adapter, push the plunger completely down toward the tip of the oral dispenser. Use 1 hand to hold the bottle upright. Insert the oral dispenser tip firmly into the opening of the bottle adapter. Step 4: Carefully turn the bottle upside down with the oral dispenser tip in place. Slowly pull the plunger down to withdraw your prescribed dose. Do not pull the plunger out of the oral dispenser (See Figure 2 ). 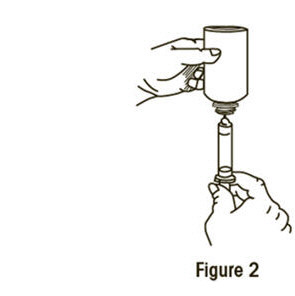
Step 5: Leave the oral dispenser tip in the bottle and turn the bottle to an upright position. Slowly remove the oral dispenser tip from the bottle.If there are air bubbles in the oral dispenser or if you have withdrawn the wrong dose, insert the oral dispenser tip back into the bottle adapter while the bottle is in an upright position. Push the plunger gently all the way up so the CELLCEPT Oral Suspension flows back into the bottle. Repeat Step 4. Step 6: Place the tip of the oral dispenser in the mouth directed towards the cheek and slowly push the plunger down until the oral dispenser is empty. Step 7: Put the child-resistant bottle cap back on the bottle and turn the cap to the right (clockwise) to close the bottle. Keep the bottle tightly closed after each use. Step 8: Rinse the oral dispenser under running tap water after each use:
- Remove the plunger from the oral dispenser.
- Rinse the oral dispenser and plunger with water only and let them air dry on a paper towel.
- When the oral dispenser and plunger are dry, put the plunger back in the oral dispenser for the next use. Do not throw away the oral dispenser. Store the oral dispenser in a clean, dry place.
- Do not boil the oral dispenser. Do not use solvent-containing wipes to clean the oral dispenser. Do not use cloths or wipes to dry the oral dispenser.
How should I store CELLCEPT Oral Suspension?
- Store the CELLCEPT Oral Suspension at room temperature between 59¬įF to 86¬įF (15¬įC to 30¬įC), for up to 60 days. You can also store the CELLCEPT Oral Suspension in the refrigerator between 36¬įF to 46¬įF (2¬įC to 8¬įC). )
- Do not freeze.
Keep CELLCEPT Oral Suspension and all medicines out of the reach of children.
Distributed by: Genentech USA, Inc. A Member of the Roche Group1 DNA WaySouth San Francisco, CA 94080-4990 ©2022 Genentech, Inc. All rights reserved.
This Instructions for Use has been approved by the U.S. Food and Drug Administration.
Revised: August 2022
Representative sample of labeling (see the HOW SUPPLIED section for complete uling):
Principal Display Panel - 500 Mg Tablet Bottle Carton
NDC 0004-0260-43
CellCept¬ģ (mycophenolate mofetil tablets)
500 mg
Each tablet contains 500 mg mycophenolate mofetil.
Rx only
Attention Pharmacist: Dispense the accompanying Medication Guide to each patient. For additional Medication Guides call 1-800-617-8191 or visit www.gene.com/gene/ products/information/cellcept.
500 tablets
Genentech
10235320
Principal Display Panel - 250 Mg Capsule Bottle Carton
NDC 0004-0259-43
CellCept¬ģ (mycophenolate mofetil capsules)
250 mg
Each capsule contains 250 mg mycophenolate mofetil.
Rx only
Attention Pharmacist: Dispense the accompanying Medication Guide to each patient. For additional Medication Guides call 1-800-617-8191 or visit www.gene.com/gene/ products/information/cellcept.
500 capsules
Genentech
10225420
Principal Display Panel - 500 Mg Vial Carton
NDC 0004-0298-09
CellCept¬ģ Intravenous (mycophenolate mofetil for injection)
500 mg
FOR INTRAVENOUS INFUSION ONLY.
Each single-dose vial contains the equivalent of 500 mg mycophenolate mofetil (equivalent to 542 mg of mycophenolate mofetil hydrochloride), 25 mg polysorbate 80 and 5 mg citric acid. Sodium hydroxide or hydrochloric acid may have been used to adjust pH.
Attention Pharmacist: Dispense the accompanying Medication Guide to each patient. For additional Medication Guides, call 1-800-617-8191 or visit www.gene.com/gene/products/information/cellcept.
Rx only 4 Single-Dose Vials
Genentech
10225424
Principal Display Panel - 200 Mg/ml Bottle Carton
NDC 0004-0261-29
CellCept¬ģ Oral Suspension (mycophenolate mofetil for oral suspension)
200 mg/mL
Each mL contains 200 mg mycophenolate mofetil after constitution.
Attention Pharmacist: Dispense the accompanyingMedication Guide to each patient. For additionalMedication Guides, call 1-800-617-8191 or visitwww.gene.com/gene/products/information/cellcept.
Rx only
Genentech
10225425
DISCLAIMER:
"This tool does not provide medical advice, and is for informational and educational purposes only, and is not a substitute for professional medical advice, treatment or diagnosis. Call your doctor to receive medical advice. If you think you may have a medical emergency, please dial 911."
"Do not rely on openFDA to make decisions regarding medical care. While we make every effort to ensure that data is accurate, you should assume all results are unvalidated. We may limit or otherwise restrict your access to the API in line with our Terms of Service."
"This product uses publicly available data from the U.S. National Library of Medicine (NLM), National Institutes of Health, Department of Health and Human Services; NLM is not responsible for the product and does not endorse or recommend this or any other product."
PillSync may earn a commission via links on our site
