Xarelto (rivaroxaban 10 mg) Dailymed
Generic: rivaroxaban is used for the treatment of Hemorrhage Pulmonary Embolism Venous Thrombosis Stroke
IMPRINT: 15 XA
SHAPE: round
COLOR: red
All Imprints
rivaroxaban 20 mg - 20 xa triangle red
rivaroxaban 20 mg - xa 20 triangle red
rivaroxaban 15 mg - xa 15 round red
xarelto (rivaroxaban) tablet, film coated xarelto (rivaroxaban) kit - 20 xa triangle red
rivaroxaban 10 mg oral tablet [xarelto] - 10 xa round red
xarelto (rivaroxaban) tablet, film coated xarelto (rivaroxaban) kit - xa 20 triangle red
rivaroxaban 2.5 mg oral tablet [xarelto] - xa 2 5 round yellow
xarelto (rivaroxaban) tablet, film coated xarelto (rivaroxaban) tablet, film coated xarelto (rivaroxaban) kit - 15 xa round red
xarelto (rivaroxaban) tablet, film coated xarelto (rivaroxaban) tablet, film coated xarelto (rivaroxaban) kit - xa 15 round red
rivaroxaban 15 mg - 15 xa round red
rivaroxaban 10 mg - 10 xa round red
Boxed Warning
Warning: (a) Premature Discontinuation Of Xarelto Increases The Risk Of Thrombotic Events, (b) Spinal/epidural Hematoma
- use of indwelling epidural catheters
- concomitant use of other drugs that affect hemostasis, such as non-steroidal anti-inflammatory drugs (NSAIDs), platelet inhibitors, other anticoagulants
- a history of traumatic or repeated epidural or spinal punctures
- a history of spinal deformity or spinal surgery
- optimal timing between the administration of XARELTO and neuraxial procedures is not known

Go PRO for all pill images
Warning: (a) Premature Discontinuation Of Xarelto Increases The Risk Of Thrombotic Events, (b) Spinal/epidural Hematoma
WARNING: (A) PREMATURE DISCONTINUATION OF XARELTO INCREASES THE RISK OF THROMBOTIC EVENTS, (B) SPINAL/EPIDURAL HEMATOMA
See full prescribing information for complete boxed warning.
(A) Premature discontinuation of XARELTO increases the risk of thrombotic events
Premature discontinuation of any oral anticoagulant, including XARELTO, increases the risk of thrombotic events. To reduce this risk, consider coverage with another anticoagulant if XARELTO is discontinued for a reason other than pathological bleeding or completion of a course of therapy. (2.2 ,2.3 ,5.1 ,14.1 )
(B) Spinal/epidural hematoma
Epidural or spinal hematomas have occurred in patients treated with XARELTO who are receiving neuraxial anesthesia or undergoing spinal puncture. These hematomas may result in long-term or permanent paralysis. (5.2 ,5.3 ,6.2 )
Monitor patients frequently for signs and symptoms of neurological impairment and if observed, treat urgently. Consider the benefits and risks before neuraxial intervention in patients who are or who need to be anticoagulated. (5.3 )
A. Premature discontinuation of XARELTO increases the risk of thrombotic events
Premature discontinuation of any oral anticoagulant, including XARELTO, increases the risk of thrombotic events. If anticoagulation with XARELTO is discontinued for a reason other than pathological bleeding or completion of a course of therapy, consider coverage with another anticoagulant [see Dosage and Administration (2.3, 2.4), Warnings and Precautions (5.1), and Clinical Studies (14.1)] .
B. Spinal/epidural hematoma
Epidural or spinal hematomas have occurred in patients treated with XARELTO who are receiving neuraxial anesthesia or undergoing spinal puncture. These hematomas may result in long-term or permanent paralysis. Consider these risks when scheduling patients for spinal procedures. Factors that can increase the risk of developing epidural or spinal hematomas in these patients include:
- use of indwelling epidural catheters
- concomitant use of other drugs that affect hemostasis, such as non-steroidal anti-inflammatory drugs (NSAIDs), platelet inhibitors, other anticoagulants
- a history of traumatic or repeated epidural or spinal punctures
- a history of spinal deformity or spinal surgery
- optimal timing between the administration of XARELTO and neuraxial procedures is not known
[see Warnings and Precautions (5.2, 5.3) and Adverse Reactions (6.2)].
Monitor patients frequently for signs and symptoms of neurological impairment. If neurological compromise is noted, urgent treatment is necessary [see Warnings and Precautions (5.3)] .
Consider the benefits and risks before neuraxial intervention in patients anticoagulated or to be anticoagulated for thromboprophylaxis [see Warnings and Precautions (5.3)] .
1 Indications And Usage
XARELTO is a factor Xa inhibitor indicated:
- to reduce risk of stroke and systemic embolism in nonvalvular atrial fibrillation (
1.1 )- for treatment of deep vein thrombosis (DVT) (
1.2 )- for treatment of pulmonary embolism (PE) (
1.3 )- for reduction in the risk of recurrence of DVT or PE (
1.4 )- for the prophylaxis of DVT, which may lead to PE in patients undergoing knee or hip replacement surgery (
1.5 )- for prophylaxis of venous thromboembolism (VTE) in acutely ill medical patients (
1.6 )- to reduce the risk of major cardiovascular events in patients with coronary artery disease (CAD) (
1.7 )- to reduce the risk of major thrombotic vascular events in patients with peripheral artery disease (PAD), including patients after recent lower extremity revascularization due to symptomatic PAD (
1.8 )- for treatment of VTE and reduction in the risk of recurrent VTE in pediatric patients from birth to less than 18 years (
1.9 )- for thromboprophylaxis in pediatric patients 2 years and older with congenital heart disease after the Fontan procedure (
1.10 )1.1Reduction of Risk of Stroke and Systemic Embolism in Nonvalvular Atrial Fibrillation
XARELTO is indicated to reduce the risk of stroke and systemic embolism in adult patients with nonvalvular atrial fibrillation.
There are limited data on the relative effectiveness of XARELTO and warfarin in reducing the risk of stroke and systemic embolism when warfarin therapy is well-controlled [see Clinical Studies (14.1)].
1.2Treatment of Deep Vein Thrombosis
XARELTO is indicated for the treatment of deep vein thrombosis (DVT).
1.3Treatment of Pulmonary Embolism
XARELTO is indicated for the treatment of pulmonary embolism (PE).
1.4Reduction in the Risk of Recurrence of Deep Vein Thrombosis and/or Pulmonary Embolism
XARELTO is indicated for the reduction in the risk of recurrence of DVT and/or PE in adult patients at continued risk for recurrent DVT and/or PE after completion of initial treatment lasting at least 6 months.
1.5Prophylaxis of Deep Vein Thrombosis Following Hip or Knee Replacement Surgery
XARELTO is indicated for the prophylaxis of DVT, which may lead to PE in adult patients undergoing knee or hip replacement surgery.
1.6Prophylaxis of Venous Thromboembolism in Acutely Ill Medical Patients at Risk for Thromboembolic Complications Not at High Risk of Bleeding
XARELTO is indicated for the prophylaxis of venous thromboembolism (VTE) and VTE related death during hospitalization and post hospital discharge in adult patients admitted for an acute medical illness who are at risk for thromboembolic complications due to moderate or severe restricted mobility and other risk factors for VTE and not at high risk of bleeding [see Warnings and Precautions (5.2) and Clinical Studies (14.5)] .
1.7Reduction of Risk of Major Cardiovascular Events in Patients with Coronary Artery Disease (CAD)
XARELTO, in combination with aspirin, is indicated to reduce the risk of major cardiovascular events (cardiovascular death, myocardial infarction, and stroke) in adult patients with coronary artery disease.
1.8Reduction of Risk of Major Thrombotic Vascular Events in Patients with Peripheral Artery Disease (PAD), Including Patients after Lower Extremity Revascularization due to Symptomatic PAD
XARELTO, in combination with aspirin, is indicated to reduce the risk of major thrombotic vascular events (myocardial infarction, ischemic stroke, acute limb ischemia, and major amputation of a vascular etiology) in adult patients with PAD, including patients who have recently undergone a lower extremity revascularization procedure due to symptomatic PAD.
1.9Treatment of Venous Thromboembolism and Reduction in Risk of Recurrent Venous Thromboembolism in Pediatric Patients
XARELTO is indicated for the treatment of venous thromboembolism (VTE) and the reduction in the risk of recurrent VTE in pediatric patients from birth to less than 18 years after at least 5 days of initial parenteral anticoagulant treatment.
1.10Thromboprophylaxis in Pediatric Patients with Congenital Heart Disease after the Fontan Procedure
XARELTO is indicated for thromboprophylaxis in pediatric patients aged 2 years and older with congenital heart disease who have undergone the Fontan procedure.
2 Dosage And Administration
- Nonvalvular Atrial Fibrillation: 15 or 20 mg, once daily with food (
2.1 )- Treatment of DVT and/or PE: 15 mg orally twice daily with food for the first 21 days followed by 20 mg orally once daily with food for the remaining treatment (
2.1 )- Reduction in the Risk of Recurrence of DVT and/or PE in patients at continued risk for DVT and/or PE: 10 mg once daily with or without food, after at least 6 months of standard anticoagulant treatment (
2.1 )- Prophylaxis of DVT Following Hip or Knee Replacement Surgery: 10 mg orally once daily with or without food (
2.1 )- Prophylaxis of VTE in Acutely Ill Medical Patients at Risk for Thromboembolic Complications Not at High Risk of Bleeding: 10 mg once daily, with or without food, in hospital and after hospital discharge for a total recommended duration of 31 to 39 days (
2.1 )- CAD or PAD: 2.5 mg orally twice daily with or without food, in combination with aspirin (75–100 mg) once daily (
2.1 )- Pediatric Patients: See dosing recommendations in the Full Prescribing Information (
2.2 )2.1Recommended Dosage in Adults
Table 1: Recommended Dosage in Adults Indication Renal Considerations Calculate CrCl based on actual weight. [See Warnings and Precautions (5.4) and Use in Specific Populations (8.6)] Dosage Food/Timing See Clinical Pharmacology (12.3) Reduction in Risk of Stroke in Nonvalvular Atrial Fibrillation CrCl >50 mL/min 20 mg once daily Take with evening meal CrCl ≤50 mL/min Patients with CrCl <30 mL/min were not studied, but administration of XARELTO is expected to result in serum concentrations of rivaroxaban similar to those in patients with moderate renal impairment (CrCl 30 to <50 mL/min) [see Use in Specific Populations (8.6)] 15 mg once daily Take with evening meal Treatment of DVT and/or PE CrCl ≥15 mL/min 15 mg twice daily ▼ after 21 days, transition to ▼ 20 mg once daily Take with food, at the same time each day CrCl <15 mL/min Avoid Use Reduction in the Risk of Recurrence of DVT and/or PE in patients at continued risk for DVT and/or PE CrCl ≥15 mL/min 10 mg once daily, after at least 6 months of standard anticoagulant treatment Take with or without food CrCl <15 mL/min Avoid Use Prophylaxis of DVT Following:
- Hip Replacement Surgery
See Dosage and Administration (2.4) CrCl ≥15 mL/min 10 mg once daily for 35 days, 6–10 hours after surgery once hemostasis has been established Take with or without food CrCl <15 mL/min Avoid Use
- Knee Replacement Surgery
CrCl ≥15 mL/min 10 mg once daily for 12 days, 6–10 hours after surgery once hemostasis has been established Take with or without food CrCl <15 mL/min Avoid Use Prophylaxis of VTE in Acutely Ill Medical Patients at Risk for Thromboembolic Complications Not at High Risk of Bleeding CrCl ≥15 mL/min 10 mg once daily, in hospital and after hospital discharge, for a total recommended duration of 31 to 39 days Take with or without food CrCl <15 mL/min Avoid Use Reduction of Risk of Major Cardiovascular Events (CV Death, MI, and Stroke) in CAD No dose adjustment needed based on CrCl 2.5 mg twice daily, plus aspirin (75–100 mg) once daily Take with or without food Reduction of Risk of Major Thrombotic Vascular Events in PAD, Including Patients after Lower Extremity Revascularization due to Symptomatic PAD No dose adjustment needed based on CrCl 2.5 mg twice daily, plus aspirin (75–100 mg) once daily. When starting therapy after a successful lower extremity revascularization procedure, initiate once hemostasis has been established. Take with or without food 2.2Recommended Dosage in Pediatric Patients
Treatment of Venous Thromboembolism and Reduction in Risk of Recurrent Venous Thromboembolism in Pediatric Patients
Table 2: Recommended Dosage in Pediatric Patients Birth to Less than 18 Years for Treatment of and Reduction in Risk of Recurrent VTE Initiate XARELTO treatment following at least 5 days of initial parenteral anticoagulation therapy. ,Patients <6 months of age should meet the following criteria: at birth were at least 37 weeks of gestation, have had at least 10 days of oral feeding, and weigh ≥2.6 kg at the time of dosing. Dosage Form Body Weight 1 mg XARELTO = 1 mL Suspension Dosage Total Daily Dose All doses should be taken with feeding or with food since exposures match that of 20 mg daily dose in adults. Once a Day Once a day: approximately 24 hours apart; 2 times a day: approximately 12 hours apart; 3 times a day: approximately 8 hours apart 2 Times a Day 3 Times a Day Oral Suspension Only 2.6 kg to 2.9 kg 0.8 mg 2.4 mg 3 kg to 3.9 kg 0.9 mg 2.7 mg 4 kg to 4.9 kg 1.4 mg 4.2 mg 5 kg to 6.9 kg 1.6 mg 4.8 mg 7 kg to 7.9 kg 1.8 mg 5.4 mg 8 kg to 8.9 kg 2.4 mg 7.2 mg 9 kg to 9.9 kg 2.8 mg 8.4 mg 10 kg to 11.9 kg 3 mg 9 mg 12 kg to 29.9 kg 5 mg 10 mg Oral Suspension or Tablets 30 kg to 49.9 kg 15 mg 15 mg ≥50 kg 20 mg 20 mg
Dosing of XARELTO was not studied and therefore dosing cannot be reliably determined in the following patient populations. Its use is therefore not recommended in children less than 6 months of age with any of the following:
- Less than 37 weeks of gestation at birth
- Less than 10 days of oral feeding
- Body weight of less than 2.6 kg.
To increase absorption, all doses should be taken with feeding or with food.
Monitor the child's weight and review the dose regularly, especially for children below 12 kg. This is to ensure a therapeutic dose is maintained.
All pediatric patients (except <2 years old with catheter-related thrombosis): Therapy with XARELTO should be continued for at least 3 months in children with thrombosis. Treatment can be extended up to 12 months when clinically necessary. The benefit of continued therapy beyond 3 months should be assessed on an individual basis taking into account the risk for recurrent thrombosis versus the potential risk of bleeding.
Pediatric patients <2 years old with catheter-related thrombosis: Therapy with XARELTO should be continued for at least 1 month in children less than 2 years old with catheter-related thrombosis. Treatment can be extended up to 3 months when clinically necessary. The benefit of continued therapy beyond 1 month should be assessed on an individual basis taking into account the risk for recurrent thrombosis versus the potential risk of bleeding.
Thromboprophylaxis in Pediatric Patients with Congenital Heart Disease after the Fontan Procedure
Table 3: Recommended Dosage for Thromboprophylaxis in Pediatric Patients with Congenital Heart Disease Dosage Form Body Weight 1 mg XARELTO = 1 mL Suspension Dosage Total Daily Dose All doses can be taken with or without food since exposures match that of 10 mg daily dose in adults. Once a Day Once a day: approximately 24 hours apart; 2 times a day: approximately 12 hours apart. 2 Times a Day Oral Suspension Only 7 kg to 7.9 kg 1.1 mg 2.2 mg 8 kg to 9.9 kg 1.6 mg 3.2 mg 10 kg to 11.9 kg 1.7 mg 3.4 mg 12 kg to 19.9 kg 2 mg 4 mg 20 kg to 29.9 kg 2.5 mg 5 mg 30 kg to 49.9 kg 7.5 mg 7.5 mg Oral Suspension or Tablets ≥50 kg 10 mg 10 mg
Administration in Pediatric Patients
Food Effect:
For the treatment of VTE in children, the dose should be taken with food to increase absorption.
For thromboprophylaxis after Fontan procedure, the dose can be taken with or without food.
Use in Renal Impairment in Pediatric Patients
Patients 1 Year of Age or Older
- Mild renal impairment (eGFR: 50 to ≤ 80 mL/min/1.73 m 2): No dose adjustment is required.
- Moderate or severe renal impairment (eGFR: <50 mL/min/1.73 m 2): avoid use, as limited clinical data are available.
Estimated glomerular filtration rate (eGFR) can be done using the updated Schwartz formula, eGFR (Schwartz) = (0.413 Ă— height in cm)/serum creatinine in mg/dL, if serum creatinine (SCr) is measured by an enzymatic creatinine method that has been calibrated to be traceable to isotope dilution mass spectrometry (IDMS).
If SCr is measured with routine methods that have not been recalibrated to be traceable to IDMS (e.g., the traditional Jaffé reaction), the eGFR should be obtained from the original Schwartz formula: eGFR (mL/min/1.73 m 2) = k * height (cm)/SCr (mg/dL), where k is proportionality constant:
- k = 0.55 in children 1 year to 13 years
- k = 0.55 in girls > 13 and < 18 years
- k = 0.70 in boys > 13 and < 18 years
Patients Less than 1 Year of Age
Determine renal function using serum creatinine. Avoid use of XARELTO in pediatric patients younger than 1 year with serum creatinine results above 97.5 th percentile, as no clinical data are available.
Table 4: Reference Values of Serum Creatinine in Pediatric Patients <1 Year of Age Age 97.5 th Percentile of Creatinine (mg/dL) 97.5 th Percentile of Creatinine (µmol/L) Week 2 0.52 46 Week 3 0.46 41 Week 4 0.42 37 Month 2 0.37 33 Month 3 0.34 30 Month 4–6 0.34 30 Month 7–9 0.34 30 Month 10–12 0.36 32 2.3Switching to and from XARELTO
Switching from Warfarin to XARELTO - When switching patients from warfarin to XARELTO, discontinue warfarin and start XARELTO as soon as the International Normalized Ratio (INR) is below 3.0 in adults and below 2.5 in pediatric patients to avoid periods of inadequate anticoagulation.
Switching from XARELTO to Warfarin –
- Adults:
No clinical trial data are available to guide converting patients from XARELTO to warfarin. XARELTO affects INR, so INR measurements made during coadministration with warfarin may not be useful for determining the appropriate dose of warfarin. One approach is to discontinue XARELTO and begin both a parenteral anticoagulant and warfarin at the time the next dose of XARELTO would have been taken.
- Pediatric Patients:
To ensure adequate anticoagulation during the transition from XARELTO to warfarin, continue XARELTO for at least 2 days after the first dose of warfarin. After 2 days of co-administration, an INR should be obtained prior to the next scheduled dose of XARELTO. Co-administration of XARELTO and warfarin is advised to continue until the INR is ≥ 2.0.
Once XARELTO is discontinued, INR testing may be done reliably 24 hours after the last dose.
2.4Discontinuation for Surgery and other Interventions
If anticoagulation must be discontinued to reduce the risk of bleeding with surgical or other procedures, XARELTO should be stopped at least 24 hours before the procedure to reduce the risk of bleeding [see Warnings and Precautions (5.2)] . In deciding whether a procedure should be delayed until 24 hours after the last dose of XARELTO, the increased risk of bleeding should be weighed against the urgency of intervention. XARELTO should be restarted after the surgical or other procedures as soon as adequate hemostasis has been established, noting that the time to onset of therapeutic effect is short [see Warnings and Precautions (5.1)] . If oral medication cannot be taken during or after surgical intervention, consider administering a parenteral anticoagulant.
2.5Missed Dose
Adults
- For patients receiving 2.5 mg twice daily: if a dose is missed, the patient should take a single 2.5 mg XARELTO dose as recommended at the next scheduled time.
- For patients receiving 15 mg twice daily: The patient should take XARELTO immediately to ensure intake of 30 mg XARELTO per day. Two 15 mg tablets may be taken at once.
- For patients receiving 20 mg, 15 mg or 10 mg once daily: The patient should take the missed XARELTO dose immediately. The dose should not be doubled within the same day to make up for a missed dose.
Pediatric Patients
- If XARELTO is taken once a day, the patient should take the missed dose as soon as possible once it is noticed, but only on the same day. If this is not possible, the patient should skip the dose and continue with the next dose as prescribed. The patient should not take two doses to make up for a missed dose.
- If XARELTO is taken two times a day, the patient should take the missed morning dose as soon as possible once it is noticed. A missed morning dose may be taken together with the evening dose. A missed evening dose can only be taken in the same evening.
- If XARELTO is taken three times a day, if a dose is missed, the patient should skip the missed dose and go back to the regular dosing schedule at the usual time without compensating for the missed dose.
On the following day, the patient should continue with their regular regimen.
2.6Administration Options
For adult patients who are unable to swallow whole tablets, XARELTO tablets (all strengths) may be crushed and mixed with applesauce immediately prior to use and administered orally. After the administration of a crushed XARELTO 15 mg or 20 mg tablet, the dose should be immediately followed by food. Administration with food is not required for the 2.5 mg or 10 mg tablets [see Clinical Pharmacology (12.3)] .
Administration of XARELTO tablets via nasogastric (NG) tube or gastric feeding tube: After confirming gastric placement of the tube, XARELTO tablets (all strengths) may be crushed and suspended in 50 mL of water and administered via an NG tube or gastric feeding tube. Since rivaroxaban absorption is dependent on the site of drug release, avoid administration of XARELTO distal to the stomach which can result in reduced absorption and thereby, reduced drug exposure. After the administration of a crushed XARELTO 15 mg or 20 mg tablet, the dose should then be immediately followed by enteral feeding. Enteral feeding is not required following administration of the 2.5 mg or 10 mg tablets [see Clinical Pharmacology (12.3)] .
Crushed XARELTO tablets (all strengths) are stable in water and in applesauce for up to 4 hours. An in vitro compatibility study indicated that there is no adsorption of rivaroxaban from a water suspension of a crushed XARELTO tablet to PVC or silicone nasogastric (NG) tubing.
Administration of XARELTO suspension via NG tube or gastric feeding tube: XARELTO oral suspension may be given through NG or gastric feeding tube. After the administration, flush the feeding tube with water.
For the treatment or reduction in risk of recurrent VTE in pediatric patients, the dose should then be immediately followed by enteral feeding to increase absorption. For the thromboprophylaxis in pediatric patients with congenital heart disease who have undergone the Fontan procedure, the dose does not require to be followed by enteral feeding.
An in vitro compatibility study indicated that XARELTO suspension can be used with PVC, polyurethane or silicone NG tubing.
2.7Preparation Instructions for Pharmacy of XARELTO for Oral Suspension
Do not add flavor as product is already flavored (sweet and creamy).
Reconstitute before dispensing:
- Tap the bottle until all granules flow freely.
- Add 150 mL of purified water for reconstitution.
- Shake for 60 seconds. Check that all granules are wetted and the suspension is uniform.
- Push the adaptor into bottleneck and recap bottle.
- The suspension must be used within 60 days.
- Write the "Discard after" date on the bottle and carton.
Dispensing Instructions:
- Dispense in the original bottle.
- Dispense the bottle upright with the syringes provided in the original carton.
Store reconstituted suspension at room temperature between 20°C to 25°C (68°F to 77°F); excursions permitted between 15°C to 30°C (59°F to 86°F). Do not freeze.
It is recommended the pharmacist counsel the caregiver on proper use. Alert the patient or caregiver to read the Medication Guide and Instructions for Use.
3 Dosage Forms And Strengths
- 2.5 mg tablets: Round, light yellow, and film-coated with a triangle pointing down above a "2.5" marked on one side and "Xa" on the other side
- 10 mg tablets: Round, light red, biconvex and film-coated with a triangle pointing down above a "10" marked on one side and "Xa" on the other side
- 15 mg tablets: Round, red, biconvex, and film-coated with a triangle pointing down above a "15" marked on one side and "Xa" on the other side
- 20 mg tablets: Triangle-shaped, dark red, and film-coated with a triangle pointing down above a "20" marked on one side and "Xa" on the other side
- For oral suspension: white to off-white granules; once reconstituted, provide flavored white to off-white opaque liquid with a concentration of 1 mg/mL.
- Tablets: 2.5 mg, 10 mg, 15 mg, and 20 mg (
3 )- For oral suspension: 1 mg/mL once reconstituted (
3 )
4 Contraindications
XARELTO is contraindicated in patients with:
- active pathological bleeding [see Warnings and Precautions (5.2)]
- severe hypersensitivity reaction to XARELTO (e.g., anaphylactic reactions) [see Adverse Reactions (6.2)]
- Active pathological bleeding (
4 )- Severe hypersensitivity reaction to XARELTO (
4 )
5 Warnings And Precautions
- Risk of bleeding: XARELTO can cause serious and fatal bleeding. An agent to reverse the activity of rivaroxaban is available. (
5.2 )- Pregnancy-related hemorrhage: Use XARELTO with caution in pregnant women due to the potential for obstetric hemorrhage and/or emergent delivery. (
5.7 ,8.1 )- Prosthetic heart valves: XARELTO use not recommended. (
5.8 )- Increased Risk of Thrombosis in Patients with Triple Positive Antiphospholipid Syndrome: XARELTO use not recommended. (
5.10 )5.1Increased Risk of Thrombotic Events after Premature Discontinuation
Premature discontinuation of any oral anticoagulant, including XARELTO, in the absence of adequate alternative anticoagulation increases the risk of thrombotic events. An increased rate of stroke was observed during the transition from XARELTO to warfarin in clinical trials in atrial fibrillation patients. If XARELTO is discontinued for a reason other than pathological bleeding or completion of a course of therapy, consider coverage with another anticoagulant [see Dosage and Administration (2.3, 2.4) and Clinical Studies (14.1)] .
5.2Risk of Bleeding
XARELTO increases the risk of bleeding and can cause serious or fatal bleeding. In deciding whether to prescribe XARELTO to patients at increased risk of bleeding, the risk of thrombotic events should be weighed against the risk of bleeding.
Promptly evaluate any signs or symptoms of blood loss and consider the need for blood replacement. Discontinue XARELTO in patients with active pathological hemorrhage. The terminal elimination half-life of rivaroxaban is 5 to 9 hours in healthy subjects aged 20 to 45 years.
Concomitant use of other drugs that impair hemostasis increases the risk of bleeding. These include aspirin, P2Y 12 platelet inhibitors, dual antiplatelet therapy, other antithrombotic agents, fibrinolytic therapy, non-steroidal anti-inflammatory drugs (NSAIDs) [see Drug Interactions (7.4)] , selective serotonin reuptake inhibitors, and serotonin norepinephrine reuptake inhibitors.
Concomitant use of drugs that are known combined P-gp and strong CYP3A inhibitors increases rivaroxaban exposure and may increase bleeding risk [see Drug Interactions (7.2)] .
Risk of Hemorrhage in Acutely Ill Medical Patients at High Risk of Bleeding
Acutely ill medical patients with the following conditions are at increased risk of bleeding with the use of XARELTO for primary VTE prophylaxis: history of bronchiectasis, pulmonary cavitation, or pulmonary hemorrhage, active cancer (i.e., undergoing acute, in-hospital cancer treatment), active gastroduodenal ulcer in the three months prior to treatment, history of bleeding in the three months prior to treatment, or dual antiplatelet therapy. XARELTO is not for use for primary VTE prophylaxis in these hospitalized, acutely ill medical patients at high risk of bleeding.
Reversal of Anticoagulant Effect
An agent to reverse the anti-factor Xa activity of rivaroxaban is available. Because of high plasma protein binding, rivaroxaban is not dialyzable [see Clinical Pharmacology (12.3)] . Protamine sulfate and vitamin K are not expected to affect the anticoagulant activity of rivaroxaban. Use of procoagulant reversal agents, such as prothrombin complex concentrate (PCC), activated prothrombin complex concentrate or recombinant factor VIIa, may be considered but has not been evaluated in clinical efficacy and safety studies. Monitoring for the anticoagulation effect of rivaroxaban using a clotting test (PT, INR or aPTT) or anti-factor Xa (FXa) activity is not recommended.
5.3Spinal/Epidural Anesthesia or Puncture
When neuraxial anesthesia (spinal/epidural anesthesia) or spinal puncture is employed, patients treated with anticoagulant agents for prevention of thromboembolic complications are at risk of developing an epidural or spinal hematoma which can result in long-term or permanent paralysis [see Boxed Warning] .
To reduce the potential risk of bleeding associated with the concurrent use of XARELTO and epidural or spinal anesthesia/analgesia or spinal puncture, consider the pharmacokinetic profile of XARELTO [see Clinical Pharmacology (12.3)] . Placement or removal of an epidural catheter or lumbar puncture is best performed when the anticoagulant effect of XARELTO is low; however, the exact timing to reach a sufficiently low anticoagulant effect in each patient is not known.
An indwelling epidural or intrathecal catheter should not be removed before at least 2 half-lives have elapsed (i.e., 18 hours in young patients aged 20 to 45 years and 26 hours in elderly patients aged 60 to 76 years), after the last administration of XARELTO [see Clinical Pharmacology (12.3)] . The next XARELTO dose should not be administered earlier than 6 hours after the removal of the catheter. If traumatic puncture occurs, delay the administration of XARELTO for 24 hours.
Should the physician decide to administer anticoagulation in the context of epidural or spinal anesthesia/analgesia or lumbar puncture, monitor frequently to detect any signs or symptoms of neurological impairment, such as midline back pain, sensory and motor deficits (numbness, tingling, or weakness in lower limbs), bowel and/or bladder dysfunction. Instruct patients to immediately report if they experience any of the above signs or symptoms. If signs or symptoms of spinal hematoma are suspected, initiate urgent diagnosis and treatment including consideration for spinal cord decompression even though such treatment may not prevent or reverse neurological sequelae.
5.4Use in Patients with Renal Impairment
Nonvalvular Atrial Fibrillation
Periodically assess renal function as clinically indicated (i.e., more frequently in situations in which renal function may decline) and adjust therapy accordingly [see Dosage and Administration (2.1)] . Consider dose adjustment or discontinuation of XARELTO in patients who develop acute renal failure while on XARELTO [see Use in Specific Populations (8.6)].
Treatment of Deep Vein Thrombosis (DVT), Pulmonary Embolism (PE), and Reduction in the Risk of Recurrence of DVT and of PE
In patients with CrCl <30 mL/min, rivaroxaban exposure and pharmacodynamic effects are increased compared to patients with normal renal function. There are limited clinical data in patients with CrCl 15 to <30 mL/min; therefore, observe closely and promptly evaluate any signs or symptoms of blood loss in these patients. There are no clinical data in patients with CrCl <15 mL/min (including patients on dialysis); therefore, avoid the use of XARELTO in these patients.
Discontinue XARELTO in patients who develop acute renal failure while on treatment [see Use in Specific Populations (8.6)] .
Prophylaxis of Deep Vein Thrombosis Following Hip or Knee Replacement Surgery
In patients with CrCl <30 mL/min, rivaroxaban exposure and pharmacodynamic effects are increased compared to patients with normal renal function. There are limited clinical data in patients with CrCl 15 to <30 mL/min; therefore, observe closely and promptly evaluate any signs or symptoms of blood loss in these patients. There are no clinical data in patients with CrCl <15 mL/min (including patients on dialysis); therefore, avoid the use of XARELTO in these patients.
Discontinue XARELTO in patients who develop acute renal failure while on treatment [see Use in Specific Populations (8.6)].
Prophylaxis of Venous Thromboembolism in Acutely Ill Medical Patients at Risk for Thromboembolic Complications Not at High Risk of Bleeding
In patients with CrCl <30 mL/min, rivaroxaban exposure and pharmacodynamic effects are increased compared to patients with normal renal function. There are limited clinical data in patients with CrCl 15 to <30 mL/min; therefore, observe closely and promptly evaluate any signs or symptoms of blood loss in these patients. There are no clinical data in patients with CrCl <15 mL/min (including patients on dialysis); therefore, avoid the use of XARELTO in these patients.
Discontinue XARELTO in patients who develop acute renal failure while on treatment [see Use in Specific Populations (8.6)].
Pediatric Patients
There are limited clinical data in pediatric patients 1 year or older with moderate or severe renal impairment (eGFR <50 mL/min/1.73 m 2); therefore, avoid the use of XARELTO in these patients.
There are no clinical data in pediatric patients younger than 1 year with serum creatinine results above 97.5 th percentile; therefore, avoid the use of XARELTO in these patients [see Dosage and Administration (2.2) and Use in Specific Populations (8.6)] .
5.5Use in Patients with Hepatic Impairment
No clinical data are available for adult patients with severe hepatic impairment.
Avoid use of XARELTO in patients with moderate (Child-Pugh B) and severe (Child-Pugh C) hepatic impairment or with any hepatic disease associated with coagulopathy since drug exposure and bleeding risk may be increased [see Use in Specific Populations (8.7)] .
No clinical data are available in pediatric patients with hepatic impairment.
5.6Use with P-gp and Strong CYP3A Inhibitors or Inducers
Avoid concomitant use of XARELTO with known combined P-gp and strong CYP3A inhibitors [see Drug Interactions (7.2)] .
Avoid concomitant use of XARELTO with drugs that are known combined P-gp and strong CYP3A inducers [see Drug Interactions (7.3)] .
5.7Risk of Pregnancy-Related Hemorrhage
In pregnant women, XARELTO should be used only if the potential benefit justifies the potential risk to the mother and fetus. XARELTO dosing in pregnancy has not been studied. The anticoagulant effect of XARELTO cannot be monitored with standard laboratory testing. Promptly evaluate any signs or symptoms suggesting blood loss (e.g., a drop in hemoglobin and/or hematocrit, hypotension, or fetal distress) [see Warnings and Precautions (5.2) and Use in Specific Populations (8.1)] .
5.8Patients with Prosthetic Heart Valves
On the basis of the GALILEO study, use of XARELTO is not recommended in patients who have had transcatheter aortic valve replacement (TAVR) because patients randomized to XARELTO experienced higher rates of death and bleeding compared to those randomized to an anti-platelet regimen. The safety and efficacy of XARELTO have not been studied in patients with other prosthetic heart valves or other valve procedures. Use of XARELTO is not recommended in patients with prosthetic heart valves.
5.9Acute PE in Hemodynamically Unstable Patients or Patients Who Require Thrombolysis or Pulmonary Embolectomy
Initiation of XARELTO is not recommended acutely as an alternative to unfractionated heparin in patients with pulmonary embolism who present with hemodynamic instability or who may receive thrombolysis or pulmonary embolectomy.
5.10Increased Risk of Thrombosis in Patients with Triple Positive Antiphospholipid Syndrome
Direct-acting oral anticoagulants (DOACs), including XARELTO, are not recommended for use in patients with triple-positive antiphospholipid syndrome (APS). For patients with APS (especially those who are triple positive [positive for lupus anticoagulant, anticardiolipin, and anti-beta 2-glycoprotein I antibodies]), treatment with DOACs has been associated with increased rates of recurrent thrombotic events compared with vitamin K antagonist therapy.
6 Adverse Reactions
The following clinically significant adverse reactions are also discussed in other sections of the labeling:
- Increased Risk of Stroke After Discontinuation in Nonvalvular Atrial Fibrillation [see Boxed Warning and Warnings and Precautions (5.1)]
- Bleeding Risk [see Warnings and Precautions (5.2, 5.4, 5.5, 5.6, 5.7)]
- Spinal/Epidural Hematoma [see Boxed Warning and Warnings and Precautions (5.3)]
- The most common adverse reaction (>5%) in adult patients was bleeding. (
6.1 )- The most common adverse reactions (>10%) in pediatric patients were bleeding, cough, vomiting, and gastroenteritis. (
6.1 )
To report SUSPECTED ADVERSE REACTIONS, contact Janssen Pharmaceuticals, Inc. at 1-800-526-7736 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
6.1 Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in clinical practice.
During clinical development for the approved indications, 34,947 adult patients were exposed to XARELTO.
Hemorrhage
The most common adverse reactions with XARELTO were bleeding complications [see Warnings and Precautions (5.2)] .
Nonvalvular Atrial Fibrillation
In the ROCKET AF trial, the most frequent adverse reactions associated with permanent drug discontinuation were bleeding events, with incidence rates of 4.3% for XARELTO vs. 3.1% for warfarin. The incidence of discontinuations for non-bleeding adverse events was similar in both treatment groups.
Table 5 shows the number of patients experiencing various types of bleeding events in the ROCKET AF trial.
Table 5: Bleeding Events in ROCKET AF Major bleeding events within each subcategory were counted once per patient, but patients may have contributed events to multiple subcategories. These events occurred during treatment or within 2 days of stopping treatment. - On Treatment Plus 2 DaysParameter XARELTO N=7111 n (%/year) Warfarin N=7125 n (%/year) XARELTO vs. Warfarin HR (95% CI) Abbreviations: HR = Hazard Ratio, CI = Confidence interval, CRNM = Clinically Relevant Non-Major. Major Bleeding Defined as clinically overt bleeding associated with a decrease in hemoglobin of ≥2 g/dL, a transfusion of ≥2 units of packed red blood cells or whole blood, bleeding at a critical site, or with a fatal outcome. 395 (3.6) 386 (3.5) 1.04 (0.90, 1.20)   Intracranial Hemorrhage (ICH) Intracranial bleeding events included intraparenchymal, intraventricular, subdural, subarachnoid and/or epidural hematoma. 55 (0.5) 84 (0.7) 0.67 (0.47, 0.93)     Hemorrhagic Stroke Hemorrhagic stroke in this table specifically refers to non-traumatic intraparenchymal and/or intraventricular hematoma in patients on treatment plus 2 days. 36 (0.3) 58 (0.5) 0.63 (0.42, 0.96)     Other ICH 19 (0.2) 26 (0.2) 0.74 (0.41, 1.34)   Gastrointestinal (GI) Gastrointestinal bleeding events included upper GI, lower GI, and rectal bleeding. 221 (2.0) 140 (1.2) 1.61 (1.30, 1.99)   Fatal Bleeding Fatal bleeding is adjudicated death with the primary cause of death from bleeding. 27 (0.2) 55 (0.5) 0.50 (0.31, 0.79)     ICH 24 (0.2) 42 (0.4) 0.58 (0.35, 0.96)     Non-intracranial 3 (0.0) 13 (0.1) 0.23 (0.07, 0.82)
Figure 1 shows the risk of major bleeding events across major subgroups.
Note: The figure above presents effects in various subgroups all of which are baseline characteristics and all of which were pre-specified (diabetic status was not pre-specified in the subgroup but was a criterion for the CHADS2 score). The 95% confidence limits that are shown do not take into account how many comparisons were made, nor do they reflect the effect of a particular factor after adjustment for all other factors. Apparent homogeneity or heterogeneity among groups should not be over-interpreted. Figure 1: Risk of Major Bleeding Events by Baseline Characteristics in ROCKET AF – On Treatment Plus 2 Days
Treatment of Deep Vein Thrombosis (DVT) and/or Pulmonary Embolism (PE)
Reduction in the Risk of Recurrence of DVT and/or PE
Prophylaxis of Deep Vein Thrombosis Following Hip or Knee Replacement Surgery
In the RECORD clinical trials, the overall incidence rate of adverse reactions leading to permanent treatment discontinuation was 3.7% with XARELTO.
The rates of major bleeding events and any bleeding events observed in patients in the RECORD clinical trials are shown in Table 8.
Table 8: Bleeding Events Bleeding events occurring any time following the first dose of double-blind study medication (which may have been prior to administration of active drug) until two days after the last dose of double-blind study medication. Patients may have more than one event. in Patients Undergoing Hip or Knee Replacement Surgeries (RECORD 1–3)XARELTO 10 mg Enoxaparin Includes the placebo-controlled period for RECORD 2, enoxaparin dosing was 40 mg once daily (RECORD 1–3) Total treated patients N=4487 n (%) N=4524 n (%)   Major bleeding event 14 (0.3) 9 (0.2)     Fatal bleeding 1 (<0.1) 0     Bleeding into a critical organ 2 (<0.1) 3 (0.1)     Bleeding that required re-operation 7 (0.2) 5 (0.1)     Extra-surgical site bleeding requiring transfusion of >2 units of whole blood or packed cells 4 (0.1) 1 (<0.1)   Any bleeding event Includes major bleeding events 261 (5.8) 251 (5.6) Hip Surgery Studies N=3281 n (%) N=3298 n (%)   Major bleeding event 7 (0.2) 3 (0.1)     Fatal bleeding 1 (<0.1) 0     Bleeding into a critical organ 1 (<0.1) 1 (<0.1)     Bleeding that required re-operation 2 (0.1) 1 (<0.1)     Extra-surgical site bleeding requiring transfusion of >2 units of whole blood or packed cells 3 (0.1) 1 (<0.1)   Any bleeding event 201 (6.1) 191 (5.8) Knee Surgery Study N=1206 n (%) N=1226 n (%)   Major bleeding event 7 (0.6) 6 (0.5)     Fatal bleeding 0 0     Bleeding into a critical organ 1 (0.1) 2 (0.2)     Bleeding that required re-operation 5 (0.4) 4 (0.3)     Extra-surgical site bleeding requiring transfusion of >2 units of whole blood or packed cells 1 (0.1) 0   Any bleeding event 60 (5.0) 60 (4.9)
Following XARELTO treatment, the majority of major bleeding complications (≥60%) occurred during the first week after surgery.
Prophylaxis of Venous Thromboembolism in Acutely Ill Medical Patients at Risk for Thromboembolic Complications Not at High Risk of Bleeding
In the MAGELLAN study, the most frequent adverse reactions associated with permanent drug discontinuation were bleeding events. Cases of pulmonary hemorrhage and pulmonary hemorrhage with bronchiectasis were observed. Patients with bronchiectasis/pulmonary cavitation, active cancer (i.e., undergoing acute, in-hospital cancer treatment), dual antiplatelet therapy or active gastroduodenal ulcer or any bleeding in the previous three months all had an excess of bleeding with XARELTO compared with enoxaparin/placebo and are excluded from all MAGELLAN data presented in Table 9. The incidence of bleeding leading to drug discontinuation was 2.5% for XARELTO vs. 1.4% for enoxaparin/placebo.
Table 9 shows the number of patients experiencing various types of bleeding events in the MAGELLAN study.
Table 9: Bleeding Events in MAGELLAN Patients at high risk of bleeding (i.e. bronchiectasis/pulmonary cavitation, active cancer, dual antiplatelet therapy or active gastroduodenal ulcer or any bleeding in the previous three months) were excluded. Study–Safety Analysis Set - On Treatment Plus 2 DaysMAGELLAN Study Patients received either XARELTO or placebo once daily for 35 ±4 days starting in hospital and continuing post hospital discharge or received enoxaparin or placebo once daily for 10 ±4 days in the hospital. XARELTO 10 mg N=3218 n (%) Enoxaparin 40 mg /placebo N=3229 n (%) Major bleeding Defined as clinically overt bleeding associated with a drop in hemoglobin of ≥2 g/dL, a transfusion of ≥2 units of packed red blood cells or whole blood, bleeding at a critical site, or with a fatal outcome. Major bleeding events within each subcategory were counted once per patient, but patients may have contributed events to multiple subcategories. These events occurred during treatment or within 2 days of stopping treatment. 22 (0.7) 15 (0.5)   Critical site bleeding 7 (0.2) 4 (0.1)   Fatal bleeding Fatal bleeding is adjudicated death with the primary cause of death from bleeding. 3 (<0.1) 1 (<0.1) Clinically relevant non-major bleeding events (CRNM) 93 (2.9) 34 (1.1)
Reduction of Risk of Major Cardiovascular Events in Patients with CAD
In the COMPASS trial overall, the most frequent adverse reactions associated with permanent drug discontinuation were bleeding events, with incidence rates of 2.7% for XARELTO 2.5 mg twice daily vs. 1.2% for placebo on background therapy for all patients with aspirin 100 mg once daily. The incidences of important bleeding events in the CAD and PAD populations in COMPASS were similar.
Table 10 shows the number of patients experiencing various types of major bleeding events in the COMPASS trial.
Table 10: Major Bleeding Events in COMPASS - On Treatment Plus 2 Days Major bleeding events within each subcategory were counted once per patient, but patients may have contributed events to multiple subcategories. These events occurred during treatment or within 2 days of stopping treatment in the safety analysis set in COMPASS patients. Parameter XARELTO Treatment schedule: XARELTO 2.5 mg twice daily or placebo. All patients received background therapy with aspirin 100 mg once daily. N=9134 n (%/year)Placebo N=9107 n (%/year) XARELTO vs. Placebo HR (95 % CI) CI: confidence interval; HR: hazard ratio; ISTH: International Society on Thrombosis and Hemostasis Modified ISTH Major Bleeding Defined as i) fatal bleeding, or ii) symptomatic bleeding in a critical area or organ, such as intraarticular, intramuscular with compartment syndrome, intraspinal, intracranial, intraocular, respiratory, pericardial, liver, pancreas, retroperitoneal, adrenal gland or kidney; or iii) bleeding into the surgical site requiring reoperation, or iv) bleeding leading to hospitalization. 263 (1.6) 144 (0.9) 1.8 (1.5, 2.3)
- Fatal bleeding event   Intracranial hemorrhage (ICH)   Non-intracranial
12 (<0.1) 6 (<0.1) 6 (<0.1) 8 (<0.1) 3 (<0.1) 5 (<0.1) 1.5 (0.6, 3.7) 2.0 (0.5, 8.0) 1.2 (0.4, 4.0)
- Symptomatic bleeding in critical organ (non-fatal)
- ICH (fatal and non-fatal)   Hemorrhagic Stroke   Other ICH
58 (0.3) 23 (0.1) 18 (0.1) 6 (<0.1) 43 (0.3) 21 (0.1) 13 (<0.1) 9 (<0.1) 1.4 (0.9, 2.0) 1.1 (0.6, 2.0) 1.4 (0.7, 2.8) 0.7 (0.2, 1.9)
- Bleeding into the surgical site requiring reoperation (non-fatal, not in critical organ)
7 (<0.1) 6 (<0.1) 1.2 (0.4, 3.5)
- Bleeding leading to hospitalization (non-fatal, not in critical organ, not requiring reoperation)
188 (1.1) 91 (0.5) 2.1 (1.6, 2.7) Major GI bleeding 117 (0.7) 49 (0.3) 2.4 (1.7, 3.4)
Reduction of Risk of Major Thrombotic Vascular Events in Patients with Peripheral Artery Disease (PAD), Including Patients after Lower Extremity Revascularization due to Symptomatic PAD
The incidence of premature permanent discontinuation due to bleeding events for XARELTO 2.5 mg twice daily vs. placebo on background therapy with aspirin 100 mg once daily in VOYAGER was 4.1% vs. 1.6% and in COMPASS PAD was 2.7% vs. 1.3%, respectively.
Table 11 shows the number of patients experiencing various types of TIMI (Thrombolysis in Myocardial Infarction) major bleeding events in the VOYAGER trial. The most common site of bleeding was gastrointestinal.
Table 11: Major Bleeding Events Major bleeding events within each subcategory were counted once per patient, but patients may have contributed events to multiple subcategories. in VOYAGER- On Treatment Plus 2 DaysXARELTO Treatment schedule: XARELTO 2.5 mg twice daily or placebo. All patients received background therapy with aspirin 100 mg once daily. N=3256Placebo N=3248 XARELTO vs. Placebo HR (95 % CI) Parameter n (%) Event rate %/year n (%) Event rate %/year CABG: Coronary artery bypass graft; CI: confidence interval; HR: hazard ratio; TIMI: Thrombolysis in Myocardial Infarction Bleeding Criteria TIMI Major Bleeding (CABG/non-CABG) 62 (1.9) 0.96 44 (1.4) 0.67 1.4 (1.0, 2.1)   Fatal bleeding 6 (0.2) 0.09 6 (0.2) 0.09 1.0 (0.3, 3.2)   Intracranial bleeding 13 (0.4) 0.20 17 (0.5) 0.26 0.8 (0.4, 1.6)   Clinically overt signs of hemorrhage associated with a drop in hemoglobin of ≥5 g/dL or drop in hematocrit of ≥15% 46 (1.4) 0.71 24 (0.7) 0.36 1.9 (1.2, 3.2)
Other Adverse Reactions
Non-hemorrhagic adverse reactions reported in ≥1% of XARELTO-treated patients in the EINSTEIN DVT and EINSTEIN PE studies are shown in Table 12.
Table 12: Other Adverse Reactions Adverse reaction with Relative Risk >1.5 for XARELTO versus comparator Reported by ≥1% of XARELTO-Treated Patients in EINSTEIN DVT and EINSTEIN PE StudiesBody System Adverse Reaction EINSTEIN DVT Study XARELTO 20 mg N=1718 n (%) Enoxaparin/VKA N=1711 n (%) Gastrointestinal disorders   Abdominal pain 46 (2.7) 25 (1.5) General disorders and administration site conditions   Fatigue 24 (1.4) 15 (0.9) Musculoskeletal and connective tissue disorders   Back pain 50 (2.9) 31 (1.8)   Muscle spasm 23 (1.3) 13 (0.8) Nervous system disorders   Dizziness 38 (2.2) 22 (1.3) Psychiatric disorders   Anxiety 24 (1.4) 11 (0.6)   Depression 20 (1.2) 10 (0.6)   Insomnia 28 (1.6) 18 (1.1) EINSTEIN PE Study XARELTO 20 mg N=2412 n (%) Enoxaparin/VKA N=2405 n (%) Skin and subcutaneous tissue disorders   Pruritus 53 (2.2) 27 (1.1)
Non-hemorrhagic adverse reactions reported in ≥1% of XARELTO-treated patients in RECORD 1–3 studies are shown in Table 13.
Table 13: Other Adverse Drug Reactions Adverse reaction occurring any time following the first dose of double-blind medication, which may have been prior to administration of active drug, until two days after the last dose of double-blind study medication Reported by ≥1% of XARELTO-Treated Patients in RECORD 1–3 StudiesBody System Adverse Reaction XARELTO 10 mg N=4487 n (%) Enoxaparin Includes the placebo-controlled period of RECORD 2, enoxaparin dosing was 40 mg once daily (RECORD 1–3) N=4524 n (%)Injury, poisoning and procedural complications   Wound secretion 125 (2.8) 89 (2.0) Musculoskeletal and connective tissue disorders   Pain in extremity 74 (1.7) 55 (1.2)   Muscle spasm 52 (1.2) 32 (0.7) Nervous system disorders   Syncope 55 (1.2) 32 (0.7) Skin and subcutaneous tissue disorders   Pruritus 96 (2.1) 79 (1.8)   Buler 63 (1.4) 40 (0.9)
Pediatric Patients
Treatment of Venous Thromboembolism and Reduction in Risk of Recurrent Venous Thromboembolism in Pediatric Patients
The safety assessment is based on data from the EINSTEIN Junior Phase 3 study in 491 patients from birth to less than 18 years of age. Patients were randomized 2:1 to receive body weight-adjusted doses of XARELTO or comparator (unfractionated heparin, low molecular weight heparin, fondaparinux or VKA).
Discontinuation due to bleeding events occurred in 6 (1.8%) patients in the XARELTO group and 3 (1.9%) patients in the comparator group.
Table 14 shows the number of patients experiencing bleeding events in the EINSTEIN Junior study. In female patients who had experienced menarche, ages 12 to <18 years of age, menorrhagia occurred in 23 (27%) female patients in the XARELTO group and 5 (10%) female patients in the comparator group.
Table 14: Bleeding Events in EINSTEIN Junior Study – Safety Analysis Set - Main Treatment Period These events occurred after randomization until 3 months of treatment (1 month for patients <2 years with central venous catheter-related VTE (CVC-VTE). Patients may have more than one event. Parameter XARELTO Treatment schedule: body weight-adjusted doses of XARELTO; randomized 2:1 (XARELTO: Comparator). N=329 n (%)Comparator Group Unfractionated heparin (UFH), low molecular weight heparin (LMWH), fondaparinux or VKA. N=162 n (%)Major bleeding Defined as clinically overt bleeding associated with a decrease in hemoglobin of ≥2 g/dL, a transfusion of ≥2 units of packed red blood cells or whole blood, bleeding at a critical site, or with a fatal outcome. 0 2 (1.2) Clinically relevant non-major bleeding Defined as clinically overt bleeding, which did not meet the criteria for major bleeding, but was associated with medical intervention, unscheduled contact with a physician, temporary cessation of treatment, discomfort for the patient, or impairment of activities of daily life. 10 (3.0) 1 (0.6) Trivial bleeding 113 (34.3) 44 (27.2) Any bleeding 119 (36.2) 45 (27.8)
Non-bleeding adverse reactions reported in ≥5% of XARELTO-treated patients are shown in Table 15.
Table 15: Other Adverse Reactions Adverse reaction with Relative Risk >1.5 for XARELTO versus comparator. Reported in XARELTO-Treated Patients by ≥5% in EINSTEIN Junior StudyAdverse Reaction XARELTO N=329 n (%) Comparator Group N=162 n (%) Pain in extremity 23 (7) 7 (4.3) Fatigue The following terms were combined: fatigue, asthenia. 23 (7) 7 (4.3)
A clinically relevant adverse reaction in XARELTO-treated patients was vomiting (10.6% in the XARELTO group vs 8% in the comparator group).
Thromboprophylaxis in Pediatric Patients with Congenital Heart Disease (CHD) after the Fontan Procedure
The data below are based on Part B of the UNIVERSE study which was designed to evaluate the safety and efficacy of XARELTO for thromboprophylaxis in 98 children with CHD after the Fontan procedure who took at least one dose of study drug. Patients in Part B were randomized 2:1 to receive either body weight-adjusted doses of XARELTO or aspirin (approximately 5 mg/kg).
Discontinuation due to bleeding events occurred in 1 (1.6%) patient in the XARELTO group and no patients in the aspirin group.
Table 16 shows the number of patients experiencing bleeding events in the UNIVERSE study.
Table 16: Bleeding Events in UNIVERSE Study - Safety Analysis Set - On Treatment Plus 2 Days Parameter XARELTO Treatment schedule: body weight-adjusted doses of XARELTO or aspirin (approximately 5 mg/kg); randomized 2:1 (XARELTO: Aspirin). N=64 n (%)Aspirin N=34 n (%) Major Bleeding Defined as clinically overt bleeding associated with a decrease in hemoglobin of ≥2 g/dL, a transfusion of the equivalent of ≥2 units of packed red blood cells or whole blood, bleeding at a critical site, or with a fatal outcome. 1 (1.6) 0   Epistaxis leading to transfusion 1 (1.6) 0 Clinically relevant non-major (CRNM) bleeding Defined as clinically overt bleeding, which did not meet the criteria for major bleeding, but was associated with medical intervention, unscheduled contact with a physician, temporary cessation of treatment, discomfort for the patient, or impairment of activities of daily life. 4 (6.3) 3 (8.8) Trivial bleeding 21 (32.8) 12 (35.3) Any bleeding 23 (35.9) 14 (41.2)
Non-bleeding adverse reactions reported in ≥5% of XARELTO-treated patients are shown in Table 17.
Table 17: Other Adverse Reactions Adverse reaction with Relative Risk >1.5 for XARELTO versus aspirin. Reported by ≥5% of XARELTO-Treated Patients in UNIVERSE Study (Part B)Adverse Reaction XARELTO N=64 n (%) Aspirin N=34 n (%) Cough 10 (15.6) 3 (8.8) Vomiting 9 (14.1) 3 (8.8) Gastroenteritis The following terms were combined: Gastroenteritis: gastroenteritis, gastroenteritis viral Rash: rash, rash maculo-papular, viral rash 8 (12.5) 1 (2.9) Rash 6 (9.4) 2 (5.9) 6.2 Postmarketing Experience
The following adverse reactions have been identified during post-approval use of XARELTO. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
Blood and lymphatic system disorders: agranulocytosis, thrombocytopenia
Hepatobiliary disorders: jaundice, cholestasis, hepatitis (including hepatocellular injury)
Immune system disorders: hypersensitivity, anaphylactic reaction, anaphylactic shock, angioedema
Nervous system disorders: hemiparesis
Renal disorders: Anticoagulant-related nephropathy
Respiratory, thoracic and mediastinal disorders: Eosinophilic pneumonia
Skin and subcutaneous tissue disorders: Stevens-Johnson syndrome, drug reaction with eosinophilia and systemic symptoms (DRESS)
7 Drug Interactions
- Avoid combined P-gp and strong CYP3A inhibitors and inducers (
7.2 ,7.3 )- Anticoagulants: Avoid concomitant use (
7.4 )7.1General Inhibition and Induction Properties
Rivaroxaban is a substrate of CYP3A4/5, CYP2J2, and the P-gp and ATP-binding cassette G2 (ABCG2) transporters. Combined P-gp and strong CYP3A inhibitors increase exposure to rivaroxaban and may increase the risk of bleeding. Combined P-gp and strong CYP3A inducers decrease exposure to rivaroxaban and may increase the risk of thromboembolic events.
7.2Drugs that Inhibit Cytochrome P450 3A Enzymes and Drug Transport Systems
Interaction with Combined P-gp and Strong CYP3A Inhibitors
Avoid concomitant administration of XARELTO with known combined P-gp and strong CYP3A inhibitors (e.g., ketoconazole and ritonavir) [see Warnings and Precautions (5.6) and Clinical Pharmacology (12.3)] .
Although clarithromycin is a combined P-gp and strong CYP3A inhibitor, pharmacokinetic data suggests that no precautions are necessary with concomitant administration with XARELTO as the change in exposure is unlikely to affect the bleeding risk [see Clinical Pharmacology (12.3)] .
Interaction with Combined P-gp and Moderate CYP3A Inhibitors in Patients with Renal Impairment
XARELTO should not be used in patients with CrCl 15 to <80 mL/min who are receiving concomitant combined P-gp and moderate CYP3A inhibitors (e.g., erythromycin) unless the potential benefit justifies the potential risk [see Warnings and Precautions (5.4) and Clinical Pharmacology (12.3)] .
7.3Drugs that Induce Cytochrome P450 3A Enzymes and Drug Transport Systems
Avoid concomitant use of XARELTO with drugs that are combined P-gp and strong CYP3A inducers (e.g., carbamazepine, phenytoin, rifampin, St. John's wort) [see Warnings and Precautions (5.6) and Clinical Pharmacology (12.3)] .
7.4Anticoagulants and NSAIDs/Aspirin
Coadministration of enoxaparin, warfarin, aspirin, clopidogrel and chronic NSAID use may increase the risk of bleeding [see Clinical Pharmacology (12.3)].
Avoid concurrent use of XARELTO with other anticoagulants due to increased bleeding risk unless benefit outweighs risk. Promptly evaluate any signs or symptoms of blood loss if patients are treated concomitantly with aspirin, other platelet aggregation inhibitors, or NSAIDs [see Warnings and Precautions (5.2)] .
8 Use In Specific Populations
- Renal impairment: Avoid or adjust dose (
8.6 )- Hepatic impairment: Avoid use in Child-Pugh B and C hepatic impairment or hepatic disease associated with coagulopathy (
8.7 )8.1 Pregnancy
Risk Summary
The limited available data on XARELTO in pregnant women are insufficient to inform a drug-associated risk of adverse developmental outcomes. Use XARELTO with caution in pregnant patients because of the potential for pregnancy related hemorrhage and/or emergent delivery. The anticoagulant effect of XARELTO cannot be reliably monitored with standard laboratory testing. Consider the benefits and risks of XARELTO for the mother and possible risks to the fetus when prescribing XARELTO to a pregnant woman [see Warnings and Precautions (5.2, 5.7)] .
Adverse outcomes in pregnancy occur regardless of the health of the mother or the use of medications. The estimated background risk of major birth defects and miscarriage for the indicated populations is unknown. In the U.S. general population, the estimated background risk of major birth defects and miscarriage in clinically recognized pregnancies is 2–4% and 15–20%, respectively.
Clinical Considerations
Disease-Associated Maternal and/or Embryo/Fetal Risk
Pregnancy is a risk factor for venous thromboembolism and that risk is increased in women with inherited or acquired thrombophilias. Pregnant women with thromboembolic disease have an increased risk of maternal complications including pre-eclampsia. Maternal thromboembolic disease increases the risk for intrauterine growth restriction, placental abruption and early and late pregnancy loss.
Fetal/Neonatal Adverse Reactions
Based on the pharmacologic activity of Factor Xa inhibitors and the potential to cross the placenta, bleeding may occur at any site in the fetus and/or neonate.
Labor or Delivery
All patients receiving anticoagulants, including pregnant women, are at risk for bleeding and this risk may be increased during labor or delivery [see Warnings and Precautions (5.7)]. The risk of bleeding should be balanced with the risk of thrombotic events when considering the use of XARELTO in this setting.
Data
Human Data
There are no adequate or well-controlled studies of XARELTO in pregnant women, and dosing for pregnant women has not been established. Post-marketing experience is currently insufficient to determine a rivaroxaban-associated risk for major birth defects or miscarriage. In an in vitro placenta perfusion model, unbound rivaroxaban was rapidly transferred across the human placenta.
Animal Data
Rivaroxaban crosses the placenta in animals. Rivaroxaban increased fetal toxicity (increased resorptions, decreased number of live fetuses, and decreased fetal body weight) when pregnant rabbits were given oral doses of ≥10 mg/kg rivaroxaban during the period of organogenesis. This dose corresponds to about 4 times the human exposure of unbound drug, based on AUC comparisons at the highest recommended human dose of 20 mg/day. Fetal body weights decreased when pregnant rats were given oral doses of 120 mg/kg during the period of organogenesis. This dose corresponds to about 14 times the human exposure of unbound drug. In rats, peripartal maternal bleeding and maternal and fetal death occurred at the rivaroxaban dose of 40 mg/kg (about 6 times maximum human exposure of the unbound drug at the human dose of 20 mg/day).
8.2 Lactation
Risk Summary
Rivaroxaban has been detected in human milk. There are insufficient data to determine the effects of rivaroxaban on the breastfed child or on milk production. Rivaroxaban and/or its metabolites were present in the milk of rats. The developmental and health benefits of breastfeeding should be considered along with the mother's clinical need for XARELTO and any potential adverse effects on the breastfed infant from XARELTO or from the underlying maternal condition (see Data) .
Data
Animal Data
Following a single oral administration of 3 mg/kg of radioactive [ 14C]-rivaroxaban to lactating rats between Day 8 to 10 postpartum, the concentration of total radioactivity was determined in milk samples collected up to 32 hours post-dose. The estimated amount of radioactivity excreted with milk within 32 hours after administration was 2.1% of the maternal dose.
8.3 Females and Males of Reproductive Potential
Females of reproductive potential requiring anticoagulation should discuss pregnancy planning with their physician.
The risk of clinically significant uterine bleeding, potentially requiring gynecological surgical interventions, identified with oral anticoagulants including XARELTO should be assessed in females of reproductive potential and those with abnormal uterine bleeding.
8.4 Pediatric Use
The safety and effectiveness of XARELTO have been established in pediatric patients from birth to less than 18 years for the treatment of VTE and the reduction in risk of recurrent VTE. Use of XARELTO is supported in these age groups by evidence from adequate and well-controlled studies of XARELTO in adults with additional pharmacokinetic, safety and efficacy data from a multicenter, prospective, open-label, active-controlled randomized study in 500 pediatric patients from birth to less than 18 years of age. XARELTO was not studied and therefore dosing cannot be reliably determined or recommended in children less than 6 months who were less than 37 weeks of gestation at birth; had less than 10 days of oral feeding, or had a body weight of less than 2.6 kg [see Dosage and Administration (2.2), Adverse Reactions (6.1), Clinical Pharmacology (12.3) and Clinical Studies (14.8)] .
The safety and effectiveness of XARELTO have been established for use in pediatric patients aged 2 years and older with congenital heart disease who have undergone the Fontan procedure. Use of XARELTO is supported in these age groups by evidence from adequate and well-controlled studies of XARELTO in adults with additional data from a multicenter, prospective, open-label, active controlled study in 112 pediatric patients to evaluate the single- and multiple-dose pharmacokinetic properties of XARELTO and the safety and efficacy of XARELTO when used for thromboprophylaxis for 12 months in children with single ventricle physiology who had the Fontan procedure [see Dosage and Administration (2.2), Adverse Reactions (6.1), Clinical Pharmacology (12.3) and Clinical Studies (14.9)] .
Clinical studies that evaluated safety, efficacy, pharmacokinetic and pharmacodynamic data support the use of XARELTO 10 mg, 15 mg, and 20 mg tablets in pediatric patients. For the XARELTO 2.5 mg tablets, there are no safety, efficacy, pharmacokinetic and pharmacodynamic data to support the use in pediatric patients. Therefore, XARELTO 2.5 mg tablets are not recommended for use in pediatric patients.
Although not all adverse reactions identified in the adult population have been observed in clinical trials of children and adolescent patients, the same warnings and precautions for adults should be considered for children and adolescents.
8.5 Geriatric Use
Of the total number of adult patients in clinical trials for the approved indications of XARELTO (N=64,943 patients), 64 percent were 65 years and over, with 27 percent 75 years and over. In clinical trials the efficacy of XARELTO in the elderly (65 years or older) was similar to that seen in patients younger than 65 years. Both thrombotic and bleeding event rates were higher in these older patients [see Clinical Pharmacology (12.3) and Clinical Studies (14)] .
8.6 Renal Impairment
In pharmacokinetic studies, compared to healthy adult subjects with normal creatinine clearance, rivaroxaban exposure increased by approximately 44 to 64% in adult subjects with renal impairment. Increases in pharmacodynamic effects were also observed [see Clinical Pharmacology (12.3)] .
Nonvalvular Atrial Fibrillation
Patients with Chronic Kidney Disease not on Dialysis
In the ROCKET AF trial, patients with CrCl 30 to 50 mL/min were administered XARELTO 15 mg once daily resulting in serum concentrations of rivaroxaban and clinical outcomes similar to those in patients with better renal function administered XARELTO 20 mg once daily. Patients with CrCl <30 mL/min were not studied, but administration of XARELTO 15 mg once daily is expected to result in serum concentrations of rivaroxaban similar to those in patients with moderate renal impairment [see Clinical Pharmacology (12.3)] .
Patients with End-Stage Renal Disease on Dialysis
Clinical efficacy and safety studies with XARELTO did not enroll patients with end-stage renal disease (ESRD) on dialysis. In patients with ESRD maintained on intermittent hemodialysis, administration of XARELTO 15 mg once daily will result in concentrations of rivaroxaban and pharmacodynamic activity similar to those observed in the ROCKET AF study [see Clinical Pharmacology (12.2, 12.3)] . It is not known whether these concentrations will lead to similar stroke reduction and bleeding risk in patients with ESRD on dialysis as was seen in ROCKET AF.
Treatment of DVT and/or PE and Reduction in the Risk of Recurrence of DVT and/or PE
In the EINSTEIN trials, patients with CrCl values <30 mL/min at screening were excluded from the studies, but administration of XARELTO is expected to result in serum concentrations of rivaroxaban similar to those in patients with moderate renal impairment (CrCl 30 to <50 mL/min) [see Clinical Pharmacology (12.3)]. Observe closely and promptly evaluate any signs or symptoms of blood loss in patients with CrCl 15 to <30 mL/min. Avoid the use of XARELTO in patients with CrCl <15 mL/min.
Prophylaxis of DVT Following Hip or Knee Replacement Surgery
The combined analysis of the RECORD 1–3 clinical efficacy studies did not show an increase in bleeding risk for patients with CrCl 30 to 50 mL/min and reported a possible increase in total venous thromboemboli in this population. In the RECORD 1–3 trials, patients with CrCl values <30 mL/min at screening were excluded from the studies, but administration of XARELTO 10 mg once daily is expected to result in serum concentrations of rivaroxaban similar to those in patients with moderate renal impairment (CrCl 30 to <50 mL/min) [see Clinical Pharmacology (12.3)]. Observe closely and promptly evaluate any signs or symptoms of blood loss in patients with CrCl 15 to <30 mL/min. Avoid the use of XARELTO in patients with CrCl <15 mL/min.
Prophylaxis of Venous Thromboembolism in Acutely Ill Medical Patients at Risk for Thromboembolic Complications Not at High Risk of Bleeding
Patients with CrCl values <30 mL/min at screening were excluded from the MAGELLAN study. In patients with CrCl <30 mL/min a dose of XARELTO 10 mg once daily is expected to result in serum concentrations of rivaroxaban similar to those in patients with moderate renal impairment (CrCl 30 to <50 mL/min) [see Clinical Pharmacology (12.3)] . Observe closely and promptly evaluate any signs or symptoms of blood loss in patients with CrCl 15 to <30 mL/min. Avoid use of XARELTO in patients with CrCl <15 mL/min.
Reduction of Risk of Major Cardiovascular Events in Patients with CAD and Reduction of Risk of Major Thrombotic Vascular Events in Patients with PAD, Including Patients After Recent Lower Extremity Revascularization due to Symptomatic PAD
Patients with Chronic Kidney Disease not on Dialysis
Patients with a CrCl <15 mL/min at screening were excluded from COMPASS and VOYAGER, and limited data are available for patients with a CrCl of 15 to 30 mL/min. In patients with CrCl <30 mL/min, a dose of 2.5 mg XARELTO twice daily is expected to give an exposure similar to that in patients with moderate renal impairment (CrCl 30 to <50 mL/min) [see Clinical Pharmacology (12.3)] , whose efficacy and safety outcomes were similar to those with preserved renal function.
Patients with End-Stage Renal Disease on Dialysis
No clinical outcome data is available for the use of XARELTO with aspirin in patients with ESRD on dialysis since these patients were not enrolled in COMPASS or VOYAGER. In patients with ESRD maintained on intermittent hemodialysis, administration of XARELTO 2.5 mg twice daily will result in concentrations of rivaroxaban and pharmacodynamic activity similar to those observed in moderate renal impaired patients in the COMPASS study [see Clinical Pharmacology (12.2, 12.3)] . It is not known whether these concentrations will lead to similar CV risk reduction and bleeding risk in patients with ESRD on dialysis as was seen in COMPASS.
Pediatric Use
No dosage adjustment is required in patients 1 year of age or older with mild renal impairment (eGFR 50 to ≤ 80 mL/min/1.73 m 2). There are limited clinical data in pediatric patients 1 year or older with moderate or severe renal impairment (eGFR <50 mL/min/1.73 m 2); therefore, avoid the use of XARELTO in these patients.
There are no clinical data in pediatric patients younger than 1 year with serum creatinine results above 97.5 th percentile; therefore, avoid the use of XARELTO in these patients [see Dosage and Administration (2.2)] .
8.7 Hepatic Impairment
In a pharmacokinetic study, compared to healthy adult subjects with normal liver function, AUC increases of 127% were observed in adult subjects with moderate hepatic impairment (Child-Pugh B).
The safety or PK of XARELTO in patients with severe hepatic impairment (Child-Pugh C) has not been evaluated [see Clinical Pharmacology (12.3)] .
Avoid the use of XARELTO in patients with moderate (Child-Pugh B) and severe (Child-Pugh C) hepatic impairment or with any hepatic disease associated with coagulopathy.
No clinical data are available in pediatric patients with hepatic impairment.
10 Overdosage
Overdose of XARELTO may lead to hemorrhage. Discontinue XARELTO and initiate appropriate therapy if bleeding complications associated with overdosage occur. Rivaroxaban systemic exposure is not further increased at single doses >50 mg due to limited absorption. The use of activated charcoal to reduce absorption in case of XARELTO overdose may be considered. Due to the high plasma protein binding, rivaroxaban is not dialyzable [see Warnings and Precautions (5.2) and Clinical Pharmacology (12.3)] . Partial reversal of laboratory anticoagulation parameters may be achieved with use of plasma products. An agent to reverse the anti-factor Xa activity of rivaroxaban is available.
11 Description
Rivaroxaban, a factor Xa (FXa) inhibitor, is the active ingredient in XARELTO ® Tablets and XARELTO ® for oral suspension with the chemical name 5-Chloro-N-({(5S)-2-oxo-3-[4-(3-oxo-4-morpholinyl)phenyl]-1,3-oxazolidin-5-yl}methyl)-2-thiophenecarboxamide. The molecular formula of rivaroxaban is C 19H 18ClN 3O 5S and the molecular weight is 435.89. The structural formula is:
Rivaroxaban is a pure ( S)-enantiomer. It is an odorless, non-hygroscopic, white to yellowish powder. Rivaroxaban is only slightly soluble in organic solvents (e.g., acetone, polyethylene glycol 400) and is practically insoluble in water and aqueous media.
Each XARELTO tablet contains 2.5 mg, 10 mg, 15 mg, or 20 mg of rivaroxaban. The inactive ingredients of XARELTO are: croscarmellose sodium, hypromellose, lactose monohydrate, magnesium stearate, microcrystalline cellulose, and sodium lauryl sulfate. Additionally, the proprietary film coating mixture used for XARELTO 2.5 mg is Opadry ® Light Yellow, containing ferric oxide yellow, hypromellose, polyethylene glycol 3350, and titanium dioxide, and for XARELTO 10 mg tablets is Opadry ® Pink and for XARELTO 15 mg tablets is Opadry ® Red, both containing ferric oxide red, hypromellose, polyethylene glycol 3350, and titanium dioxide, and for XARELTO 20 mg tablets is Opadry ® II Dark Red, containing ferric oxide red, polyethylene glycol 3350, polyvinyl alcohol (partially hydrolyzed), talc, and titanium dioxide.
XARELTO for oral suspension is supplied as granules in bottles containing 155 mg of rivaroxaban (1 mg of rivaroxaban per mL after reconstitution). The inactive ingredients are: anhydrous citric acid, hypromellose, mannitol, microcrystalline cellulose and carboxymethylcellulose sodium, sodium benzoate, sucralose, sweet and creamy flavor and xanthan gum.
12 Clinical Pharmacology
12.1 Mechanism of Action
XARELTO is a selective inhibitor of FXa. It does not require a cofactor (such as Anti-thrombin III) for activity. Rivaroxaban inhibits free FXa and prothrombinase activity. Rivaroxaban has no direct effect on platelet aggregation, but indirectly inhibits platelet aggregation induced by thrombin. By inhibiting FXa, rivaroxaban decreases thrombin generation.
12.2 Pharmacodynamics
Rivaroxaban produces dose-dependent inhibition of FXa activity. Clotting tests, such as prothrombin time (PT), activated partial thromboplastin time (aPTT) and HepTest ®, are also prolonged dose-dependently. In children treated with rivaroxaban, the correlation between anti-factor Xa to plasma concentrations is linear with a slope close to 1.
Monitoring for anticoagulation effect of rivaroxaban using anti-FXa activity or a clotting test is not recommended.
Specific Populations
Renal Impairment
The relationship between systemic exposure and pharmacodynamic activity of rivaroxaban was altered in adult subjects with renal impairment relative to healthy control subjects [see Use in Specific Populations (8.6)] .
Table 18: Percentage Increase in Rivaroxaban PK and PD Measures in Adult Subjects with Renal Impairment Relative to Healthy Subjects from Clinical Pharmacology Studies Measure Parameter Creatinine Clearance (mL/min) 50–79 30–49 15–29 ESRD (on dialysis) Separate stand-alone study. ESRD (post-dialysis) PT = Prothrombin time; FXa = Coagulation factor Xa; AUC = Area under the plasma concentration-time curve; AUEC = Area under the effect-time curve Exposure AUC 44 52 64 47 56 FXa Inhibition AUEC 50 86 100 49 33 PT Prolongation AUEC 33 116 144 112 158
Hepatic Impairment
Anti-Factor Xa activity was similar in adult subjects with normal hepatic function and in mild hepatic impairment (Child-Pugh A class). There is no clear understanding of the impact of hepatic impairment beyond this degree on the coagulation cascade and its relationship to efficacy and safety.
12.3 Pharmacokinetics
Absorption
The absolute bioavailability of rivaroxaban is dose-dependent. For the 2.5 mg and 10 mg dose, it is estimated to be 80% to 100% and is not affected by food. XARELTO 2.5 mg and 10 mg tablets can be taken with or without food. XARELTO 20 mg administered in the fasted state has an absolute bioavailability of approximately 66%. Coadministration of XARELTO with food increases the bioavailability of the 20 mg dose (mean AUC and C max increasing by 39% and 76% respectively with food). XARELTO 15 mg and 20 mg tablets should be taken with food [see Dosage and Administration (2.1)] .
The maximum concentrations (C max) of rivaroxaban appear 2 to 4 hours after tablet intake. The pharmacokinetics of rivaroxaban were not affected by drugs altering gastric pH. Coadministration of XARELTO (30 mg single dose) with the H 2-receptor antagonist ranitidine (150 mg twice daily), the antacid aluminum hydroxide/magnesium hydroxide (10 mL) or XARELTO (20 mg single dose) with the PPI omeprazole (40 mg once daily) did not show an effect on the bioavailability and exposure of rivaroxaban (see Figure 3).
Absorption of rivaroxaban is dependent on the site of drug release in the GI tract. A 29% and 56% decrease in AUC and C max compared to tablet was reported when rivaroxaban granulate is released in the proximal small intestine. Exposure is further reduced when drug is released in the distal small intestine, or ascending colon. Avoid administration of rivaroxaban distal to the stomach which can result in reduced absorption and related drug exposure.
In a study with 44 healthy subjects, both mean AUC and C max values for 20 mg rivaroxaban administered orally as a crushed tablet mixed in applesauce were comparable to that after the whole tablet. However, for the crushed tablet suspended in water and administered via an NG tube followed by a liquid meal, only mean AUC was comparable to that after the whole tablet, and C max was 18% lower.
Distribution
Protein binding of rivaroxaban in human plasma is approximately 92% to 95%, with albumin being the main binding component. The steady-state volume of distribution in healthy subjects is approximately 50 L.
Metabolism
Approximately 51% of an orally administered [ 14C]-rivaroxaban dose was recovered as inactive metabolites in urine (30%) and feces (21%). Oxidative degradation catalyzed by CYP3A4/5 and CYP2J2 and hydrolysis are the major sites of biotransformation. Unchanged rivaroxaban was the predominant moiety in plasma with no major or active circulating metabolites.
Excretion
In a Phase 1 study, following the administration of [ 14C]-rivaroxaban, approximately one-third (36%) was recovered as unchanged drug in the urine and 7% was recovered as unchanged drug in feces. Unchanged drug is excreted into urine, mainly via active tubular secretion and to a lesser extent via glomerular filtration (approximate 5:1 ratio). Rivaroxaban is a substrate of the efflux transporter proteins P-gp and ABCG2 (also abbreviated BCRP). Rivaroxaban's affinity for influx transporter proteins is unknown.
Rivaroxaban is a low-clearance drug, with a systemic clearance of approximately 10 L/hr in healthy volunteers following intravenous administration. The terminal elimination half-life of rivaroxaban is 5 to 9 hours in healthy subjects aged 20 to 45 years.
Specific Populations
The effects of level of renal impairment, age, body weight, and level of hepatic impairment on the pharmacokinetics of rivaroxaban are summarized in Figure 2.
Figure 2: Effect of Specific Adult Populations on the Pharmacokinetics of Rivaroxaban
[See Dosage and Administration (2.1)]
Gender
Gender did not influence the pharmacokinetics or pharmacodynamics of XARELTO.
Race
Healthy Japanese subjects were found to have 20 to 40% on average higher exposures compared to other ethnicities including Chinese. However, these differences in exposure are reduced when values are corrected for body weight.
Elderly
The terminal elimination half-life is 11 to 13 hours in the elderly subjects aged 60 to 76 years [see Use in Specific Populations (8.5)] .
Pediatric Patients
The rate and extent of absorption were similar between the tablet and suspension. After repeated administration of rivaroxaban for the treatment of VTE, the C max of rivaroxaban in plasma was observed at median times of 1.5 to 2.2 hours in subjects who ranged from birth to less than 18 years of age.
In children who were 6 months to 9 years of age, in vitro plasma protein binding of rivaroxaban is approximately 90%.
The half-life of rivaroxaban in plasma of pediatric patients treated for VTE decreased with decreasing age. Mean half-life values were 4.2 hours in adolescents, 3 hours in children 2 to 12 years of age, 1.9 hours in children 0.5 to <2 years of age, and 1.6 hours in children <0.5 years of age.
An exploratory analysis in pediatric patients treated for VTE did not reveal relevant differences in rivaroxaban exposure based on gender or race.
Renal Impairment
The safety and pharmacokinetics of single-dose XARELTO (10 mg) were evaluated in a study in healthy subjects [CrCl ≥80 mL/min (n=8)] and in subjects with varying degrees of renal impairment (see Figure 2). Compared to healthy subjects with normal creatinine clearance, rivaroxaban exposure increased in subjects with renal impairment. Increases in pharmacodynamic effects were also observed [see Use in Specific Populations (8.6)] .
Hepatic Impairment
The safety and pharmacokinetics of single-dose XARELTO (10 mg) were evaluated in a study in healthy adult subjects (n=16) and adult subjects with varying degrees of hepatic impairment (see Figure 2). No patients with severe hepatic impairment (Child-Pugh C) were studied. Compared to healthy subjects with normal liver function, significant increases in rivaroxaban exposure were observed in subjects with moderate hepatic impairment (Child-Pugh B) (see Figure 2). Increases in pharmacodynamic effects were also observed [see Use in Specific Populations (8.7)] .
No clinical data are available in pediatric patients with hepatic impairment.
Drug Interactions
In vitro studies indicate that rivaroxaban neither inhibits the major cytochrome P450 enzymes CYP1A2, 2C8, 2C9, 2C19, 2D6, 2J2, and 3A nor induces CYP1A2, 2B6, 2C19, or 3A. In vitro data also indicates a low rivaroxaban inhibitory potential for P-gp and ABCG2 transporters.
The effects of coadministered drugs on the pharmacokinetics of rivaroxaban exposure are summarized in Figure 3 [see Drug Interactions (7)] .
Figure 3: Effect of Coadministered Drugs on the Pharmacokinetics of Rivaroxaban in Adults
Anticoagulants
In a drug interaction study, single doses of enoxaparin (40 mg subcutaneous) and XARELTO (10 mg) given concomitantly resulted in an additive effect on anti-factor Xa activity. In another study, single doses of warfarin (15 mg) and XARELTO (5 mg) resulted in an additive effect on factor Xa inhibition and PT. Neither enoxaparin nor warfarin affected the pharmacokinetics of rivaroxaban (see Figure 3).
NSAIDs/Aspirin
In ROCKET AF, concomitant aspirin use (almost exclusively at a dose of 100 mg or less) during the double-blind phase was identified as an independent risk factor for major bleeding. NSAIDs are known to increase bleeding, and bleeding risk may be increased when NSAIDs are used concomitantly with XARELTO. Neither naproxen nor aspirin affected the pharmacokinetics of rivaroxaban (see Figure 3).
Clopidogrel
In two drug interaction studies where clopidogrel (300 mg loading dose followed by 75 mg daily maintenance dose) and XARELTO (15 mg single dose) were coadministered in healthy subjects, an increase in bleeding time to 45 minutes was observed in approximately 45% and 30% of subjects in these studies, respectively. The change in bleeding time was approximately twice the maximum increase seen with either drug alone. There was no change in the pharmacokinetics of either drug.
Drug-Disease Interactions with Drugs that Inhibit Cytochrome P450 3A Enzymes and Drug Transport Systems
In a pharmacokinetic trial, XARELTO was administered as a single dose in subjects with mild (CrCl = 50 to 79 mL/min) or moderate renal impairment (CrCl = 30 to 49 mL/min) receiving multiple doses of erythromycin (a combined P-gp and moderate CYP3A inhibitor). Compared to XARELTO administered alone in subjects with normal renal function (CrCl >80 mL/min), subjects with mild and moderate renal impairment concomitantly receiving erythromycin reported a 76% and 99% increase in AUC inf and a 56% and 64% increase in C max, respectively. Similar trends in pharmacodynamic effects were also observed.
12.6QT/QTc Prolongation
In a thorough QT study in healthy men and women aged 50 years and older, no QTc prolonging effects were observed for XARELTO (15 mg and 45 mg, single-dose).
13 Non-clinical Toxicology
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
Rivaroxaban was not carcinogenic when administered by oral gavage to mice or rats for up to 2 years. The systemic exposures (AUCs) of unbound rivaroxaban in male and female mice at the highest dose tested (60 mg/kg/day) were 1- and 2-times, respectively, the human exposure of unbound drug at the human dose of 20 mg/day. Systemic exposures of unbound drug in male and female rats at the highest dose tested (60 mg/kg/day) were 2- and 4-times, respectively, the human exposure.
Rivaroxaban was not mutagenic in bacteria (Ames-Test) or clastogenic in V79 Chinese hamster lung cells in vitro or in the mouse micronucleus test in vivo.
No impairment of fertility was observed in male or female rats when given up to 200 mg/kg/day of rivaroxaban orally. This dose resulted in exposure levels, based on the unbound AUC, at least 13 times the exposure in humans given 20 mg rivaroxaban daily.
14 Clinical Studies
14.1Stroke Prevention in Nonvalvular Atrial Fibrillation
The evidence for the efficacy and safety of XARELTO was derived from Rivaroxaban Once-daily oral direct factor Xa inhibition Compared with vitamin K antagonist for the prevention of stroke and Embolism Trial in Atrial Fibrillation (ROCKET AF) [NCT00403767], a multi-national, double-blind study comparing XARELTO (at a dose of 20 mg once daily with the evening meal in patients with CrCl >50 mL/min and 15 mg once daily with the evening meal in patients with CrCl 30 to 50 mL/min) to warfarin (titrated to INR 2.0 to 3.0) to reduce the risk of stroke and non-central nervous system (CNS) systemic embolism in patients with nonvalvular atrial fibrillation (AF). Patients had to have one or more of the following additional risk factors for stroke:
- a prior stroke (ischemic or unknown type), transient ischemic attack (TIA) or non-CNS systemic embolism, or
- 2 or more of the following risk factors:
- age ≥75 years,
- hypertension,
- heart failure or left ventricular ejection fraction ≤35%, or
- diabetes mellitus
ROCKET AF was a non-inferiority study designed to demonstrate that XARELTO preserved more than 50% of warfarin's effect on stroke and non-CNS systemic embolism as established by previous placebo-controlled studies of warfarin in atrial fibrillation.
A total of 14264 patients were randomized and followed on study treatment for a median of 590 days. The mean age was 71 years and the mean CHADS 2 score was 3.5. The population was 60% male, 83% Caucasian, 13% Asian and 1.3% Black. There was a history of stroke, TIA, or non-CNS systemic embolism in 55% of patients, and 38% of patients had not taken a vitamin K antagonist (VKA) within 6 weeks at time of screening. Concomitant diseases of patients in this study included hypertension 91%, diabetes 40%, congestive heart failure 63%, and prior myocardial infarction 17%. At baseline, 37% of patients were on aspirin (almost exclusively at a dose of 100 mg or less) and few patients were on clopidogrel. Patients were enrolled in Eastern Europe (39%); North America (19%); Asia, Australia, and New Zealand (15%); Western Europe (15%); and Latin America (13%). Patients randomized to warfarin had a mean percentage of time in the INR target range of 2.0 to 3.0 of 55%, lower during the first few months of the study.
In ROCKET AF, XARELTO was demonstrated non-inferior to warfarin for the primary composite endpoint of time to first occurrence of stroke (any type) or non-CNS systemic embolism [HR (95% CI): 0.88 (0.74, 1.03)], but superiority to warfarin was not demonstrated. There is insufficient experience to determine how XARELTO and warfarin compare when warfarin therapy is well-controlled.
Table 19 displays the overall results for the primary composite endpoint and its components.
Table 19: Primary Composite Endpoint Results in ROCKET AF Study (Intent-to-Treat Population) XARELTO Warfarin XARELTO vs. Warfarin Event N=7081 n (%) Event Rate (per 100 Pt-yrs) N=7090 n (%) Event Rate (per 100 Pt-yrs) Hazard Ratio (95% CI) Primary Composite Endpoint The primary endpoint was the time to first occurrence of stroke (any type) or non-CNS systemic embolism. Data are shown for all randomized patients followed to site notification that the study would end. 269 (3.8) 2.1 306 (4.3) 2.4 0.88 (0.74, 1.03) Stroke 253 (3.6) 2.0 281 (4.0) 2.2 Â Â Hemorrhagic Stroke Defined as primary hemorrhagic strokes confirmed by adjudication in all randomized patients followed up to site notification 33 (0.5) 0.3 57 (0.8) 0.4 Â Â Ischemic Stroke 206 (2.9) 1.6 208 (2.9) 1.6 Â Â Unknown Stroke Type 19 (0.3) 0.2 18 (0.3) 0.1 Non-CNS Systemic Embolism 20 (0.3) 0.2 27 (0.4) 0.2
Figure 4 is a plot of the time from randomization to the occurrence of the first primary endpoint event in the two treatment arms.
Figure 4: Time to First Occurrence of Stroke (any type) or Non-CNS Systemic Embolism by Treatment Group (Intent-to-Treat Population)
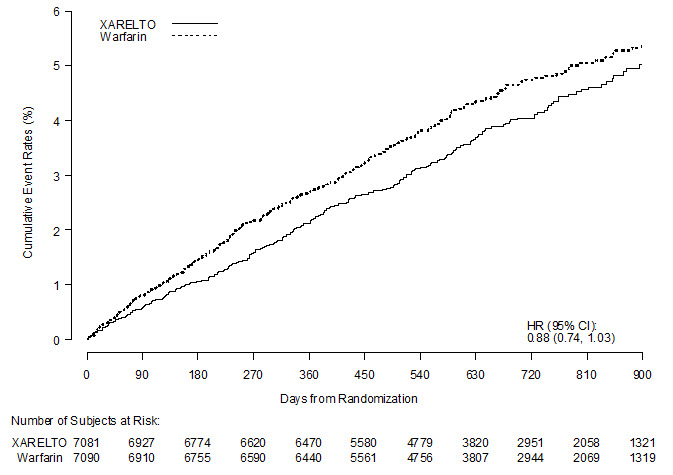
Figure 5 shows the risk of stroke or non-CNS systemic embolism across major subgroups.
Note: The figure above presents effects in various subgroups all of which are baseline characteristics and all of which were pre-specified (diabetic status was not pre-specified in the subgroup, but was a criterion for the CHADS2 score). The 95% confidence limits that are shown do not take into account how many comparisons were made, nor do they reflect the effect of a particular factor after adjustment for all other factors. Apparent homogeneity or heterogeneity among groups should not be over-interpreted.
Figure 5: Risk of Stroke or Non-CNS Systemic Embolism by Baseline Characteristics in ROCKET AFData are shown for all randomized patients followed to site notification that the study would end. (Intent-to-Treat Population)
The efficacy of XARELTO was generally consistent across major subgroups.
The protocol for ROCKET AF did not stipulate anticoagulation after study drug discontinuation, but warfarin patients who completed the study were generally maintained on warfarin. XARELTO patients were generally switched to warfarin without a period of coadministration of warfarin and XARELTO, so that they were not adequately anticoagulated after stopping XARELTO until attaining a therapeutic INR. During the 28 days following the end of the study, there were 22 strokes in the 4637 patients taking XARELTO vs. 6 in the 4691 patients taking warfarin.
Few patients in ROCKET AF underwent electrical cardioversion for atrial fibrillation. The utility of XARELTO for preventing post-cardioversion stroke and systemic embolism is unknown.
14.2Treatment of Deep Vein Thrombosis (DVT) and/or Pulmonary Embolism (PE)
EINSTEIN Deep Vein Thrombosis and EINSTEIN Pulmonary Embolism Studies
XARELTO for the treatment of DVT and/or PE was studied in EINSTEIN DVT [NCT00440193] and EINSTEIN PE [NCT00439777], multi-national, open-label, non-inferiority studies comparing XARELTO (at an initial dose of 15 mg twice daily with food for the first three weeks, followed by XARELTO 20 mg once daily with food) to enoxaparin 1 mg/kg twice daily for at least five days with VKA and then continued with VKA only after the target INR (2.0–3.0) was reached. Patients who required thrombectomy, insertion of a caval filter, or use of a fibrinolytic agent and patients with creatinine clearance <30 mL/min, significant liver disease, or active bleeding were excluded from the studies. The intended treatment duration was 3, 6, or 12 months based on investigator's assessment prior to randomization.
A total of 8281 (3449 in EINSTEIN DVT and 4832 in EINSTEIN PE) patients were randomized and followed on study treatment for a mean of 208 days in the XARELTO group and 204 days in the enoxaparin/VKA group. The mean age was approximately 57 years. The population was 55% male, 70% Caucasian, 9% Asian and about 3% Black. About 73% and 92% of XARELTO-treated patients in the EINSTEIN DVT and EINSTEIN PE studies, respectively, received initial parenteral anticoagulant treatment for a median duration of 2 days. Enoxaparin/VKA-treated patients in the EINSTEIN DVT and EINSTEIN PE studies received initial parenteral anticoagulant treatment for a median duration of 8 days. Aspirin was taken as on treatment concomitant antithrombotic medication by approximately 12% of patients in both treatment groups. Patients randomized to VKA had an unadjusted mean percentage of time in the INR target range of 2.0 to 3.0 of 58% in EINSTEIN DVT study and 60% in EINSTEIN PE study, with the lower values occurring during the first month of the study.
In the EINSTEIN DVT and EINSTEIN PE studies, 49% of patients had an idiopathic DVT/PE at baseline. Other risk factors included previous episode of DVT/PE (19%), recent surgery or trauma (18%), immobilization (16%), use of estrogen-containing drug (8%), known thrombophilic conditions (6%), or active cancer (5%).
In the EINSTEIN DVT and EINSTEIN PE studies, XARELTO was demonstrated to be non-inferior to enoxaparin/VKA for the primary composite endpoint of time to first occurrence of recurrent DVT or non-fatal or fatal PE [EINSTEIN DVT HR (95% CI): 0.68 (0.44, 1.04); EINSTEIN PE HR (95% CI): 1.12 (0.75, 1.68)]. In each study the conclusion of non-inferiority was based on the upper limit of the 95% confidence interval for the hazard ratio being less than 2.0.
Table 20 displays the overall results for the primary composite endpoint and its components for EINSTEIN DVT and EINSTEIN PE studies.
Table 20: Primary Composite Endpoint Results For the primary efficacy analysis, all confirmed events were considered from randomization up to the end of intended treatment duration (3, 6 or 12 months) irrespective of the actual treatment duration. If the same patient had several events, the patient may have been counted for several components. in EINSTEIN DVT and EINSTEIN PE Studies – Intent-to-Treat PopulationEvent XARELTO 20 mg Treatment schedule in EINSTEIN DVT and EINSTEIN PE studies: XARELTO 15 mg twice daily for 3 weeks followed by 20 mg once daily; enoxaparin/VKA [enoxaparin: 1 mg/kg twice daily, VKA: individually titrated doses to achieve a target INR of 2.5 (range: 2.0–3.0)] Enoxaparin/VKA XARELTO vs. Enoxaparin/VKA Hazard Ratio (95% CI) EINSTEIN DVT Study N=1731 n (%) N=1718 n (%) Primary Composite Endpoint 36 (2.1) 51 (3.0) 0.68 (0.44, 1.04)   Death (PE) 1 (<0.1) 0   Death (PE cannot be excluded) 3 (0.2) 6 (0.3)   Symptomatic PE and DVT 1 (<0.1) 0   Symptomatic recurrent PE only 20 (1.2) 18 (1.0)   Symptomatic recurrent DVT only 14 (0.8) 28 (1.6) EINSTEIN PE Study N=2419 n (%) N=2413 n (%) Primary Composite Endpoint 50 (2.1) 44 (1.8) 1.12 (0.75, 1.68)   Death (PE) 3 (0.1) 1 (<0.1)   Death (PE cannot be excluded) 8 (0.3) 6 (0.2)   Symptomatic PE and DVT 0 2 (<0.1)   Symptomatic recurrent PE only 23 (1.0) 20 (0.8)   Symptomatic recurrent DVT only 18 (0.7) 17 (0.7)
Figures 6 and 7 are plots of the time from randomization to the occurrence of the first primary efficacy endpoint event in the two treatment groups in EINSTEIN DVT and EINSTEIN PE studies, respectively.
Figure 6: Time to First Occurrence of the Composite of Recurrent DVT or Non-fatal or Fatal PE by Treatment Group (Intent-to-Treat Population) – EINSTEIN DVT Study
Figure 7: Time to First Occurrence of the Composite of Recurrent DVT or Non-fatal or Fatal PE by Treatment Group (Intent-to-Treat Population) – EINSTEIN PE Study
14.3Reduction in the Risk of Recurrence of DVT and/or PE
EINSTEIN CHOICE Study
XARELTO for reduction in the risk of recurrence of DVT and of PE was evaluated in the EINSTEIN CHOICE study [NCT02064439], a multi-national, double-blind, superiority study comparing XARELTO (10 or 20 mg once daily with food) to 100 mg acetylsalicylic acid (aspirin) once daily in patients who had completed 6 to 12 months of anticoagulant treatment for DVT and/or PE following the acute event. The intended treatment duration in the study was up to 12 months. Patients with an indication for continued therapeutic-dose anticoagulation were excluded.
Because the benefit-risk assessment favored the 10 mg dose versus aspirin compared to the 20 mg dose versus aspirin, only the data concerning the 10 mg dose is discussed below.
A total of 2275 patients were randomized and followed on study treatment for a mean of 290 days for the XARELTO and aspirin treatment groups. The mean age was approximately 59 years. The population was 56% male, 70% Caucasian, 14% Asian and 3% Black. In the EINSTEIN CHOICE study, 51% of patients had DVT only, 33% had PE only, and 16% had PE and DVT combined. Other risk factors included idiopathic VTE (43%), previous episode of DVT/PE (17%), recent surgery or trauma (12%), prolonged immobilization (10%), use of estrogen containing drugs (5%), known thrombophilic conditions (6%), Factor V Leiden gene mutation (4%), or active cancer (3%).
In the EINSTEIN CHOICE study, XARELTO 10 mg was demonstrated to be superior to aspirin 100 mg for the primary composite endpoint of time to first occurrence of recurrent DVT or non-fatal or fatal PE.
Table 21 displays the overall results for the primary composite endpoint and its components.
Table 21: Primary Composite Endpoint and its Components Results For the primary efficacy analysis, all confirmed events were considered from randomization up to the end of intended treatment duration (12 months) irrespective of the actual treatment duration. The individual component of the primary endpoint represents the first occurrence of the event. in EINSTEIN CHOICE Study – Full Analysis SetEvent XARELTO 10 mg N=1,127 n (%) Acetylsalicylic Acid (Aspirin) 100 mg N=1,131 n (%) XARELTO 10 mg vs. Aspirin 100 mg Hazard Ratio (95% CI) Primary Composite Endpoint 13 (1.2) 50 (4.4) 0.26 (0.14, 0.47) p<0.0001   Symptomatic recurrent DVT 8 (0.7) 29 (2.6)   Symptomatic recurrent PE 5 (0.4) 19 (1.7)   Death (PE) 0 1 (<0.1)   Death (PE cannot be excluded) 0 1 (<0.1)
Figure 8 is a plot of the time from randomization to the occurrence of the first primary efficacy endpoint event in the two treatment groups.
Figure 8: Time to First Occurrence of the Composite of Recurrent DVT or Non-fatal or Fatal PE by Treatment Group (Full Analysis Set) – EINSTEIN CHOICE Study
14.4Prophylaxis of Deep Vein Thrombosis Following Hip or Knee Replacement Surgery
XARELTO was studied in 9011 patients (4487 XARELTO-treated, 4524 enoxaparin-treated patients) in the REgulation of Coagulation in ORthopedic Surgery to Prevent DVT and PE, Controlled, Double-blind, Randomized Study of BAY 59-7939 in the Extended Prevention of VTE in Patients Undergoing Elective Total Hip or Knee Replacement (RECORD 1, 2, and 3) [NCT00329628, NCT00332020, NCT00361894] studies.
The two randomized, double-blind, clinical studies (RECORD 1 and 2) in patients undergoing elective total hip replacement surgery compared XARELTO 10 mg once daily starting at least 6 to 8 hours (about 90% of patients dosed 6 to 10 hours) after wound closure versus enoxaparin 40 mg once daily started 12 hours preoperatively. In RECORD 1 and 2, a total of 6727 patients were randomized and 6579 received study drug. The mean age [± standard deviation (SD)] was 63 ± 12.2 (range 18 to 93) years with 49% of patients ≥65 years and 55% of patients were female. More than 82% of patients were White, 7% were Asian, and less than 2% were Black. The studies excluded patients undergoing staged bilateral total hip replacement, patients with severe renal impairment defined as an estimated creatinine clearance <30 mL/min, or patients with significant liver disease (hepatitis or cirrhosis). In RECORD 1, the mean exposure duration (± SD) to active XARELTO and enoxaparin was 33.3 ± 7.0 and 33.6 ± 8.3 days, respectively. In RECORD 2, the mean exposure duration to active XARELTO and enoxaparin was 33.5 ± 6.9 and 12.4 ± 2.9 days, respectively. After Day 13, oral placebo was continued in the enoxaparin group for the remainder of the double-blind study duration. The efficacy data for RECORD 1 and 2 are provided in Table 22.
Table 22: Summary of Key Efficacy Analysis Results for Patients Undergoing Total Hip Replacement Surgery - Modified Intent-to-Treat Population RECORD 1 RECORD 2 Treatment Dosage and Duration XARELTO 10 mg once daily Enoxaparin 40 mg once daily RRR Relative Risk Reduction; CI = confidence interval , p-valueXARELTO 10 mg once daily Enoxaparin Includes the placebo-controlled period of RECORD 2 40 mg once dailyRRR , p-value Number of Patients N=1513 N=1473 N=834 N=835 Total VTE 17 (1.1%) 57 (3.9%) 71% (95% CI: 50, 83), p<0.001 17 (2.0%) 70 (8.4%) 76% (95% CI: 59, 86), p<0.001 Components of Total VTE Â Â Proximal DVT 1 (0.1%) 31 (2.1%) 5 (0.6%) 40 (4.8%) Â Â Distal DVT 12 (0.8%) 26 (1.8%) 11 (1.3%) 43 (5.2%) Â Â Non-fatal PE 3 (0.2%) 1 (0.1%) 1 (0.1%) 4 (0.5%) Â Â Death (any cause) 4 (0.3%) 4 (0.3%) 2 (0.2%) 4 (0.5%) Number of Patients N=1600 N=1587 N=928 N=929 Major VTE Proximal DVT, nonfatal PE or VTE-related death 3 (0.2%) 33 (2.1%) 91% (95% CI: 71, 97), p<0.001 6 (0.7%) 45 (4.8%) 87% (95% CI: 69, 94), p<0.001 Number of Patients N=2103 N=2119 N=1178 N=1179 Symptomatic VTE 5 (0.2%) 11 (0.5%) 3 (0.3%) 15 (1.3%)
One randomized, double-blind, clinical study (RECORD 3) in patients undergoing elective total knee replacement surgery compared XARELTO 10 mg once daily started at least 6 to 8 hours (about 90% of patients dosed 6 to 10 hours) after wound closure versus enoxaparin. In RECORD 3, the enoxaparin regimen was 40 mg once daily started 12 hours preoperatively. The mean age (± SD) of patients in the study was 68 ± 9.0 (range 28 to 91) years with 66% of patients ≥65 years. Sixty-eight percent (68%) of patients were female. Eighty-one percent (81%) of patients were White, less than 7% were Asian, and less than 2% were Black. The study excluded patients with severe renal impairment defined as an estimated creatinine clearance <30 mL/min or patients with significant liver disease (hepatitis or cirrhosis). The mean exposure duration (± SD) to active XARELTO and enoxaparin was 11.9 ± 2.3 and 12.5 ± 3.0 days, respectively. The efficacy data are provided in Table 23.
Table 23: Summary of Key Efficacy Analysis Results for Patients Undergoing Total Knee Replacement Surgery - Modified Intent-to-Treat Population RECORD 3 Treatment Dosage and Duration XARELTO 10 mg once daily Enoxaparin 40 mg once daily RRR Relative Risk Reduction; CI = confidence interval , p-valueNumber of Patients N=813 N=871 Total VTE 79 (9.7%) 164 (18.8%) 48% (95% CI: 34, 60), p<0.001 Components of events contributing to Total VTE Â Â Proximal DVT 9 (1.1%) 19 (2.2%) Â Â Distal DVT 74 (9.1%) 154 (17.7%) Â Â Non-fatal PE 0 4 (0.5%) Â Â Death (any cause) 0 2 (0.2%) Number of Patients N=895 N=917 Major VTE Proximal DVT, nonfatal PE or VTE-related death 9 (1.0%) 23 (2.5%) 60% (95% CI: 14, 81), p = 0.024 Number of Patients N=1206 N=1226 Symptomatic VTE 8 (0.7%) 24 (2.0%) 14.5Prophylaxis of Venous Thromboembolism in Acutely Ill Medical Patients at Risk for Thromboembolic Complications Not at High Risk of Bleeding
The efficacy and safety of XARELTO for prophylaxis of venous thromboembolism in acutely ill medical patients at risk for thromboembolic complications not at high risk of bleeding was evaluated in the MAGELLAN study ( Multicenter, r Andomized, parallel Group Efficacy and safety study for the prevention of venous thromboembolism in hospitalized medically i LL patients comparing rivaroxab aN with enoxaparin [NCT00571649]). MAGELLAN was a multicenter, randomized, double-blind, parallel-group efficacy and safety study comparing XARELTO to enoxaparin, in the prevention of VTE in hospitalized acutely ill medical patients during the in-hospital and post-hospital discharge period. Eligible patients included adults who were at least 40 years of age, hospitalized for an acute medical illness, at risk of VTE due to moderate or severe immobility, and had additional risk factors for VTE. The population at risk of VTE was required to have one or more of the following VTE risk factors, i.e. prolonged immobilization, age ≥75 years, history of cancer, history of VTE, history of heart failure, thrombophilia, acute infectious disease contributing to the hospitalization and BMI ≥35 kg/m 2). The causes for hospitalization included heart failure, active cancer, acute ischemic stroke, acute infectious and inflammatory disease and acute respiratory insufficiency. Patients were randomized to receive either XARELTO 10 mg once daily for 35 ±4 days starting in hospital and continuing post hospital discharge (n=4050) or enoxaparin 40 mg once daily for 10 ±4 days starting in hospital followed by placebo post-discharge (n=4051).
The major efficacy outcome in the MAGELLAN trial was a composite endpoint that included asymptomatic proximal deep venous thrombosis (DVT) in lower extremity, symptomatic proximal or distal DVT in the lower extremity, symptomatic non-fatal pulmonary embolism (PE), and death related to venous thromboembolism (VTE).
A total of 6024 patients were evaluable for the major efficacy outcome analysis (2967 on XARELTO 10 mg once daily and 3057 on enoxaparin/placebo). The mean age was 68.9 years, with 37.1% of the subject population ≥ 75 years. VTE risk factors included severe immobilization at study entry (99.9%), D-dimer > 2× ULN (43.7%), history of heart failure (35.6%), BMI ≥ 35 kg/m 2 (15.2%), chronic venous insufficiency (14.9%), acute infectious disease (13.9%), severe varicosis (12.5%), history of cancer (16.2%), history of VTE (4.5%), hormone replacement therapy (1.1%), and thrombophilia (0.3%), recent major surgery (0.8%) and recent serious trauma (0.2%). The population was 54.7% male, 68.2% White, 20.4% Asian, 1.9% Black and 5.3% Other. Admitting diagnoses for hospitalization were acute infectious diseases (43.8%) followed by congestive heart failure NYHA class III or IV (33.2%), acute respiratory insufficiency (26.4%), acute ischemic stroke (18.5%) and acute inflammatory diseases (3.4%).
Table 24 shows the overall results from the prespecified, modified intent-to-treat (mITT) analysis for the efficacy outcomes and their components. This analysis excludes approximately 25% of the patients mainly due to no ultrasonographic assessment (13.5%), inadequate assessment at day 35 (8.1%), or lack of intake of study medication (1.3%).
Table 24: Efficacy Results at Day 35 (modified Intent-to-Treat) and at Day 10 (per protocol) in the MAGELLAN Study mITT: modified intent-to-treat; PP: per protocol; DVT: Deep vein thrombosis; PE: pulmonary embolism; VTE: venous thromboembolism; CI: Confidence Interval; RR: Relative Risk Events from Day 1 to Day 35, mITT analysis set XARELTO 10 mg N=2967 n (%) Enoxaparin 40 mg/placebo N=3057 n (%) RR (95% CI) Primary Composite Endpoint at Day 35 131 (4.4%) 175 (5.7%) 0.77 (0.62, 0.96) Â Â Symptomatic non-fatal PE 10 (0.3) 14 (0.5) Â Â Symptomatic DVT in lower extremity 13 (0.4) 15 (0.5) Â Â Asymptomatic proximal DVT in lower extremity 103 (3.5) 133 (4.4) Â Â VTE related death 19 (0.6) 30 (1.0) Events from Day 1 to Day 10, PP analysis set XARELTO 10 mg N=2938 n (%) Enoxaparin 40 mg N=2993 n (%) RR (95% CI) Primary Composite Endpoint at Day 10 78 (2.7) 82 (2.7) 0.97 (0.71, 1.31) Â Â Symptomatic non-fatal PE 6 (0.2) 2 (<0.1) Â Â Symptomatic DVT in lower extremity 7 (0.2) 6 (0.2) Â Â Asymptomatic proximal DVT in lower extremity 71 (2.4) 71 (2.4) Â Â VTE related death 3 (0.1) 6 (0.2) mITT analysis set plus all-cause mortality N=3096 n (%) N=3169 n (%) RR (95% CI) Other Composite Endpoint at Day 35 266 (8.6) 293 (9.2) 0.93 (0.80, 1.09) Â Â Symptomatic non-fatal PE 10 (0.3) 14 (0.4) Â Â Symptomatic DVT in lower extremity 13 (0.4) 15 (0.5) Â Â Asymptomatic proximal DVT in lower extremity 103 (3.3) 133 (4.2) Â Â All-cause mortality 159 (5.1) 153 (4.8)
Patients with bronchiectasis/pulmonary cavitation, active cancer, dual antiplatelet therapy or active gastroduodenal ulcer or any bleeding in the previous three months (19.4%) all had an excess of bleeding with XARELTO compared with enoxaparin/placebo. Therefore, patients meeting these criteria were excluded from the following analyses presented below.
Table 25 provides the efficacy results for the subgroup of patients not at a high risk of bleeding.
Table 25: Efficacy Results at Day 35 (modified Intent-to-Treat) and at Day 10 (per protocol) in patients not at a high risk of bleeding in the MAGELLAN Study Patients at high risk of bleeding (i.e. bronchiectasis/pulmonary cavitation, active cancer, dual antiplatelet therapy or active gastroduodenal ulcer or any bleeding in the previous three months) were excluded. mITT: modified intent-to-treat; PP: per protocol; DVT: Deep vein thrombosis; PE: pulmonary embolism; VTE: venous thromboembolism; CI: Confidence Interval; RR: Relative Risk Events from Day 1 to Day 35, mITT analysis set XARELTO 10 mg N=2419 n (%) Enoxaparin 40 mg/placebo N=2506 n (%) RR (95% CI) Primary Composite Endpoint at Day 35 94 (3.9) 143 (5.7) 0.68 (0.53, 0.88) Â Â Symptomatic non-fatal PE 7 (0.3) 10 (0.4) Â Â Symptomatic DVT in lower extremity 9 (0.4) 10 (0.4) Â Â Asymptomatic proximal DVT in lower extremity 73 (3.0) 110 (4.4) Â Â VTE related death 15 (0.6) 26 (1.0) Events from Day 1 to Day 10, PP analysis set XARELTO 10 mg N=2385 n (%) Enoxaparin 40 mg N=2433 n (%) RR (95% CI) Primary Composite Endpoint at Day 10 58 (2.4) 72 (3.0) 0.82 (0.58, 1.15) Â Â Symptomatic non-fatal PE 5 (0.2) 2 (<0.1) Â Â Symptomatic DVT in lower extremity 6 (0.3) 4 (0.2) Â Â Asymptomatic proximal DVT in lower extremity 52 (2.2) 62 (2.5) Â Â VTE related death 2 (<0.1) 6 (0.2) mITT analysis set plus all-cause mortality N=2504 n (%) N=2583 n (%) RR (95% CI) Other Composite Endpoint at Day 35 184 (7.3) 225 (8.7) 0.84 (0.70, 1.02) Â Â Symptomatic non-fatal PE 7 (0.3) 10 (0.4) Â Â Symptomatic DVT in lower extremity 9 (0.4) 10 (0.4) Â Â Asymptomatic proximal DVT in lower extremity 73 (2.9) 110 (4.3) Â Â All-cause mortality 107 (4.3) 112 (4.3) 14.6Reduction of Risk of Major Cardiovascular Events in Patients with CAD
The evidence for the efficacy and safety of XARELTO for the reduction in the risk of stroke, myocardial infarction, or cardiovascular death in patients with coronary artery disease (CAD) or peripheral artery disease (PAD) was derived from the double-blind, placebo-controlled Cardiovascular Outco Mes for People using Anticoagulation Strategie S trial (COMPASS) [NCT10776424]. A total of 27,395 patients were evenly randomized to rivaroxaban 2.5 mg orally twice daily plus aspirin 100 mg once daily, rivaroxaban 5 mg orally twice daily alone, or aspirin 100 mg once daily alone. Because the 5 mg dose alone was not superior to aspirin alone, only the data concerning the 2.5 mg dose plus aspirin are discussed below.
Patients with established CAD or PAD were eligible. Patients with CAD who were younger than 65 years of age were also required to have documentation of atherosclerosis involving at least two vascular beds or to have at least two additional cardiovascular risk factors (current smoking, diabetes mellitus, an estimated glomerular filtration rate [eGFR] <60 mL per minute, heart failure, or non-lacunar ischemic stroke ≥1 month earlier). Patients with PAD were either symptomatic with ankle brachial index <0.90 or had asymptomatic carotid artery stenosis ≥50%, a previous carotid revascularization procedure, or established ischemic disease of one or both lower extremities. Patients were excluded for use of dual antiplatelet, other non-aspirin antiplatelet, or oral anticoagulant therapies, ischemic, non-lacunar stroke within 1 month, hemorrhagic or lacunar stroke at any time, or eGFR <15 mL/min.
The mean age was 68 years and 21% of the subject population were ≥75 years. Of the included patients, 91% had CAD (and will be referred to as the COMPASS CAD population), 27% had PAD (and will be referred to as the COMPASS PAD population), and 18% had both CAD and PAD. Of the patients with CAD, 69% had prior MI, 60% had prior percutaneous transluminal coronary angioplasty (PTCA)/atherectomy/ percutaneous coronary intervention (PCI), and 26% had history of coronary artery bypass grafting (CABG) prior to study. Of the patients with PAD, 49% had intermittent claudication, 27% had peripheral artery bypass surgery or peripheral percutaneous transluminal angioplasty, 26% had asymptomatic carotid artery stenosis > 50%, and 4% had limb or foot amputation for arterial vascular disease.
The mean duration of follow-up was 23 months. Relative to placebo, XARELTO reduced the rate of the primary composite outcome of stroke, myocardial infarction or cardiovascular death: HR 0.76 (95% CI: 0.66, 0.86; p=0.00004). In the COMPASS CAD population, the benefit was observed early with a constant treatment effect over the entire treatment period (see Table 26 and Figure 10).
A benefit-risk analysis of the data from COMPASS was performed by comparing the number of CV events (CV deaths, myocardial infarctions and non-hemorrhagic strokes) prevented to the number of fatal or life-threatening bleeding events (fatal bleeds + symptomatic non-fatal bleeds into a critical organ) in the XARELTO group versus the placebo group. Compared to placebo, during 10,000 patient-years of treatment, XARELTO would be expected to result in 70 fewer CV events and 12 additional life-threatening bleeds, indicating a favorable balance of benefits and risks.
The results in the COMPASS CAD population were consistent across major subgroups (see Figure 9).
Figure 9: Risk of Primary Efficacy Outcome by Baseline Characteristics in the COMPASS CAD Population (Intent-to-Treat Population)All patients received aspirin 100 mg once daily as background therapy.
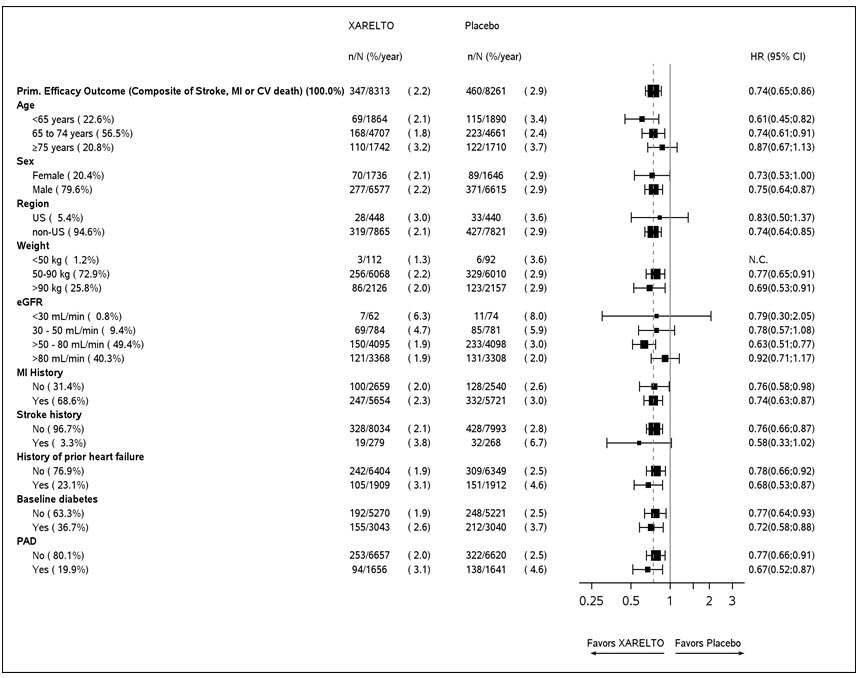
Table 26: Efficacy results from COMPASS CAD Population intention to treat analysis set, primary analyses. Event XARELTO Treatment schedule: XARELTO 2.5 mg twice daily vs placebo. All patients received aspirin 100 mg once daily as background therapy. N=8313Placebo N=8261 Hazard Ratio (95% CI) XARELTO vs. placebo. n (%) Event Rate (%/year) n (%) Event Rate (%/year) CHD: coronary heart disease, CI: confidence interval; CV: cardiovascular; MI: myocardial infarction Stroke, MI or CV death 347 (4.2) 2.2 460 (5.6) 2.9 0.74 (0.65, 0.86) - Stroke 74 (0.9) 0.5 130 (1.6) 0.8 0.56 (0.42, 0.75) - MI 169 (2.0) 1.1 195 (2.4) 1.2 0.86 (0.70, 1.05) - CV death 139 (1.7) 0.9 184 (2.2) 1.1 0.75 (0.60, 0.93) Coronary heart disease death, MI, ischemic stroke, acute limb ischemia 299 (3.6) 1.9 411 (5.0) 2.6 0.72 (0.62, 0.83) - Coronary heart disease death Coronary heart disease death: death due to acute MI, sudden cardiac death, or CV procedure. 80 (1.0) 0.5 107 (1.3) 0.7 0.74 (0.55, 0.99) - Ischemic stroke 56 (0.7) 0.3 114 (1.4) 0.7 0.49 (0.35, 0.67) - Acute limb ischemia Acute limb ischemia is defined as limb-threatening ischemia leading to an acute vascular intervention (i.e., pharmacologic, peripheral arterial surgery/reconstruction, peripheral angioplasty/stent, or amputation). 13 (0.2) 0.1 27 (0.3) 0.2 0.48 (0.25, 0.93) CV death, CV death includes CHD death, or death due to other CV causes or unknown death. MI, ischemic stroke, acute limb ischemia349 (4.2) 2.2 470 (5.7) 3.0 0.73 (0.64, 0.84) All-cause mortality 262 (3.2) 1.6 339 (4.1) 2.1 0.77 (0.65, 0.90)
CI: confidence interval
Figure 10: Time to First Occurrence of Primary Efficacy Outcome (Stroke, Myocardial Infarction, Cardiovascular Death) in the COMPASS CAD PopulationAll patients received aspirin 100 mg once daily as background therapy.
14.7Reduction of Risk of Major Thrombotic Vascular Events in Patients with PAD, Including Patients after Lower Extremity Revascularization due to Symptomatic PAD
The efficacy and safety of XARELTO 2.5 mg orally twice daily versus placebo on a background of aspirin 100 mg once daily in patients with PAD were evaluated in the COMPASS study (n=4996) and will be referred to as the COMPASS PAD population [see Clinical Studies (14.6)] .
The efficacy and safety of XARELTO were also evaluated for the reduction in the risk of the composite endpoint of myocardial infarction, ischemic stroke, cardiovascular death, acute limb ischemia (ALI), and major amputation of a vascular etiology in patients undergoing a lower extremity infrainguinal revascularization procedure due to symptomatic peripheral artery disease (PAD) in the double-blinded, placebo-controlled Vascular Outcomes stud Y of ASA alon G with rivaroxaban in Endovascular or surgical limb Revascularization for peripheral artery disease (PAD) trial (VOYAGER) [NCT02504216]. A total of 6,564 patients were equally randomized to XARELTO 2.5 mg orally twice daily vs placebo on a background therapy of aspirin 100 mg once daily.
Eligible patients included adults who were at least 50 years of age with documented moderate to severe symptomatic lower extremity atherosclerotic PAD who had a successful peripheral surgical procedure and/or endovascular procedure with or without clopidogrel (up to a maximum of 6 months was allowed; median duration of therapy was 31 days). Patients had either a prior history of limb revascularization with ankle brachial index ≤0.85 or no prior history of limb revascularization with ankle brachial index ≤0.80. Patients in need of dual antiplatelet for >6 months, or any additional antiplatelet other than aspirin and clopidogrel, or oral anticoagulant, as well as patients with a history of intracranial hemorrhage, stroke, or transient ischemic attack (TIA), or patients with eGFR <15 mL/min were excluded.
The mean age was 67 years and 20% of the subject population was ≥75 years. Of the included patients, 35% had surgical revascularization, 47% had endovascular revascularization with clopidogrel, and 18% endovascular revascularization without clopidogrel. The median duration of follow-up was 30.8 months.
XARELTO 2.5 mg twice daily was superior to placebo in reducing the rate of the primary composite outcome of myocardial infarction, ischemic stroke, cardiovascular death, acute limb ischemia (ALI), and major amputation of a vascular etiology. The primary efficacy outcome and its components are provided in Table 27. The Kaplan-Meier plot for the primary efficacy outcome can be seen in Figure 11. The secondary efficacy outcomes were tested for superiority in a prespecified, hierarchical order and the first five of seven endpoints were significantly reduced in the rivaroxaban treatment arm (see Table 27). Compared to placebo during 10,000 patient-years of treatment, XARELTO would be expected to result in 181 fewer primary outcome events and 29 more TIMI major bleeding events, indicating a favorable balance of benefits and risks.
Figure 11: Time to First Occurrence of Primary Efficacy Outcome (Myocardial Infarction, Ischemic Stroke, Cardiovascular Death, Acute Limb Ischemia, Major Amputation due to Vascular Origins) in VOYAGER All patients received aspirin 100 mg once daily as background therapy.
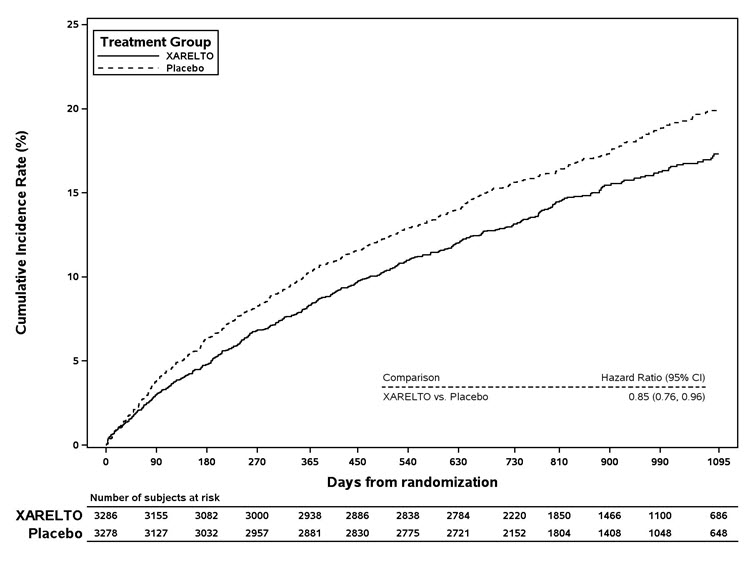
Figure 12 shows the risk of primary efficacy outcome across major subgroups. Subgroup analyses must be interpreted cautiously, as differences can reflect the play of chance among a large number of analyses. The primary efficacy endpoint generally shows homogeneous results across subgroups.
Figure 12: Risk of Primary Efficacy Outcome by Baseline Characteristics in VOYAGER (Intent-to-Treat Population)All patients received aspirin 100 mg once daily as background therapy.
Table 27 provides the efficacy event rates for the prespecified endpoints in VOYAGER and similar endpoints in the COMPASS PAD population.
Table 27: Efficacy Results in VOYAGER (Intent-to-Treat Population) and COMPASS PAD VOYAGER COMPASS PAD XARELTO N=3286 Placebo N=3278 Hazard Ratio (95% CI) XARELTO vs. placebo. p-valueTwo-sided p-values XARELTO N=2492 Placebo N=2504 Hazard Ratio (95% CI) Outcome Components Event Rate (%/year) Event Rate (%/year) Efficacy endpoints in COMPASS PAD were analysed according to the pre-specified endpoints in VOYAGER when applicable. ALI=acute limb ischemia, CHD=coronary heart disease; CI=confidence interval, CV=cardiovascular; MI=myocardial infarction, VTE=venous thromboembolism. 5-Component Outcome (Major thrombotic vascular events) Major thrombotic vascular event is the composite of MI, ischemic stroke, CV death, ALI, and major amputation of a vascular etiology. 6.8 8.0 0.85 (0.76, 0.96) p=0.0085 3.4 4.8 0.71 (0.57, 0.87) Â Â MI 1.7 1.9 0.88 (0.70, 1.12) 1.1 1.5 0.76 (0.53, 1.09) Â Â Ischemic Stroke Ischemic stroke for VOYAGER included stroke of uncertain/unknown etiology whereas COMPASS only included ischemic stroke. 0.9 1.0 0.87 (0.63, 1.19) 0.5 0.9 0.55 (0.33, 0.93) Â Â CV death CV death includes Coronary Heart Disease death, or death due to other CV causes or sudden cardiac arrest and unknown death. 2.5 2.2 1.14 (0.93, 1.40) 1.4 1.7 0.82 (0.59, 1.14) Â Â ALI 2.0 3.0 0.67 (0.55, 0.82) 0.4 0.8 0.56 (0.32, 0.99) Â Â Major amputation of a vascular etiology Adjudicated events in VOYAGER and investigator reported events in COMPASS 1.3 1.5 0.89 (0.68, 1.16) 0.2 0.6 0.40 (0.20, 0.79) VOYAGER Secondary Efficacy Outcomes Secondary outcomes for VOYAGER were tested sequentially. MI, ischemic stroke, CHD death, CHD death includes death due to sudden cardiac death, MI, or coronary revascularization procedure ALI, and major amputation due to vascular etiology5.8 7.3 0.80 (0.71, 0.91) p=0.0008 2.8 4.2 0.66 (0.53, 0.83) Unplanned index limb revascularization for recurrent limb ischemia Unplanned index limb revascularization for recurrent limb ischemia was not captured in COMPASS study. 8.4 9.5 0.88 (0.79, 0.99) p=0.028 N/A N/A N/A Hospitalization for a coronary or peripheral cause of a thrombotic nature 3.5 4.8 0.72 (0.62, 0.85) p<0.0001 1.7 2.9 0.58 (0.44, 0.77) MI, ischemic stroke, all-cause mortality, ALI, and major amputation due to vascular etiology 8.2 9.3 0.89 (0.79, 0.99) p=0.029 4.8 6.0 0.80 (0.67, 0.96) MI, all-cause stroke, CV death, ALI, and major amputation due to vascular etiology 6.9 8.1 0.86 (0.76, 0.96) p=0.010 3.4 4.9 0.70 (0.57, 0.86) All-cause mortality 4.0 3.7 1.08 (0.92, 1.27) 2.8 3.1 0.91 (0.72, 1.16) VTE events Investigator reported in VOYAGER and adjudicated events in COMPASS 0.3 0.5 0.61 (0.37, 1.00) 0.2 0.3 0.67 (0.30, 1.49) 14.8Treatment of Venous Thromboembolism and Reduction in Risk of Recurrent Venous Thromboembolism in Pediatric Patients
XARELTO for the treatment of venous thromboembolism (VTE) and reduction in the risk of recurrent VTE was evaluated in the EINSTEIN Junior Phase 3 study [NCT02234843], a multicenter, open-label, active-controlled, randomized study in 500 pediatric patients from birth to less than 18 years with confirmed VTE. There were 276 children aged 12 to <18 years, 101 children aged 6 to <12 years, 69 children aged 2 to <6 years, and 54 children aged <2 years. Patients <6 months of age were excluded from enrollment if they were <37 weeks of gestation at birth, or had <10 days of oral feeding, or had a body weight of <2.6 kg.
Index VTE was classified as either central venous catheter-related VTE (CVC-VTE), cerebral vein and sinus thrombosis (CVST), and all other VTE including DVT and PE (non-CVC-VTE).
Patients received initial treatment with therapeutic dosages of unfractionated heparin (UFH), low molecular weight heparin (LMWH), or fondaparinux for at least 5 days, and were randomized 2:1 to receive either body weight-adjusted doses of XARELTO (exposures to match that of 20 mg daily dose in adults) or comparator group (UFH, LMWH, fondaparinux or VKA) for a main study treatment period of 3 months (or 1 month for children <2 years with CVC-VTE). A diagnostic imaging test was obtained at baseline and at the end of the main study treatment. When clinically necessary, treatment was extended up to 12 months in total (or up to 3 months in total for children <2 years with CVC-VTE).
Table 28 displays the primary and secondary efficacy results.
Table 28: Efficacy Results in EINSTEIN Junior Study – Full Analysis Set Event XARELTO Treatment schedule: body weight-adjusted doses of XARELTO (exposures to match that of 20 mg daily dose in adults); randomized 2:1 (XARELTO: Comparator). N=335 n (%) (95% CI)Confidence intervals for incidence proportion were calculated by applying the method of Blyth-Still-Casella. Comparator Group Unfractionated heparin (UFH), low molecular weight heparin (LMWH), fondaparinux or VKA. N=165 n (%) (95% CI)XARELTO vs. Comparator Group Risk Difference (95% CI) Confidence intervals for difference in incidence proportions were calculated by unstratified exact method according to Agresti-Min using the standardized test statistic and inverting a two-sided test. XARELTO vs. Comparator Group Hazard Ratio (95% CI) Primary efficacy outcome: Symptomatic recurrent VTE 4 (1.2) (0.4%, 3.0%) 5 (3.0) (1.2%, 6.6%) -1.8% (-6.0%, 0.6%) 0.40 (0.11, 1.41) Secondary efficacy outcome: Symptomatic recurrent VTE or asymptomatic deterioration on repeat imaging 5 (1.5) (0.6%, 3.4%) 6 (3.6) (1.6%, 7.6%) -2.1% (-6.5%, 0.6%)
Complete resolution of thrombus on repeat imaging without recurrent VTE occurred in 128 of 335 children (38.2%, 95% CI 33.0%, 43.5%) in the XARELTO group and 43 of 165 children (26.1%, 95% CI 19.8%, 33.0%) in the comparator group. Symptomatic recurrent VTE or major bleeding events occurred in 4 of 335 children (1.2%, 95% CI 0.4%, 3.0%) in the XARELTO group and 7 of 165 children (4.2%, 95% CI 2.0%, 8.4%) in the comparator group.
14.9Thromboprophylaxis in Pediatric Patients with Congenital Heart Disease after the Fontan Procedure
The efficacy and safety of XARELTO for thromboprophylaxis in pediatric patients with congenital heart disease who have undergone the Fontan procedure was evaluated in the UNIVERSE Phase 3 study [NCT02846532]. UNIVERSE was a prospective, open-label, active controlled, multicenter, 2-part study, designed to evaluate the single- and multiple-dose pharmacokinetic properties of XARELTO (Part A), and to evaluate the safety and efficacy of XARELTO when used for thromboprophylaxis for 12 months compared with aspirin (Part B) in children 2 to 8 years of age with single ventricle physiology who had the Fontan procedure. Patients in Part B were randomized 2:1 to receive either body weight-adjusted doses of XARELTO (exposures to match that of 10 mg daily dose in adults) or aspirin (approximately 5 mg/kg). Patients with eGFR <30 ml/min/1.73 m 2 were excluded.
The median time between Fontan procedure and the first dose of XARELTO was 4 (range: 2–61) days in Part A and 34 (range: 2–124) days in part B. In comparison, the median time to initiating aspirin was 24 (range 2–117) days.
Table 29 displays the primary efficacy results.
Table 29: Efficacy Results in UNIVERSE Study – Full Analysis Set Part A Part A: single arm; not randomized Part B Part B: randomized 2:1 (XARELTO: Aspirin) Event XARELTO N=12 n (%) (95% CI) Confidence intervals for incidence proportion were calculated by applying the method of Blyth-Still-Casella. XARELTO Treatment schedule: body weight-adjusted doses of XARELTO (exposures to match that of 10 mg daily dose in adults) or aspirin (approximately 5 mg/kg) N=64 n (%) (95% CI)Aspirin N=34 n (%) (95% CI) XARELTO vs. Aspirin Risk Difference (95% CI) Confidence intervals for difference in incidence proportions were calculated by unstratified exact method according to Agresti-Min using the standardized test statistic and inverting a two-sided test. Primary efficacy outcome: any thrombotic event 1 (8.3) (0.4%, 34.9%) 1 (1.6) (0.1%, 7.8%) 3 (8.8) (2.4%, 22.2%) -7.3% (-21.7%, 1.1%) Ischemic stroke 0 (0.0%, 23.6%) 0 (0.0%, 5.6%) 1 (2.9) 0.2%, 15.1%) -2.9% (-16.2%, 2.9%) Pulmonary embolism 0 (0.0%, 23.6%) 1 (1.6) (0.1%, 7.8%) 0 (0.0%, 9.0%) 1.6% (-9.9%, 8.4%) Venous thrombosis 1 (8.3) (0.4%, 34.9%) 0 (0.0%, 5.6%) 2 (5.9) (1.1%, 18.8%) -5.9% (-20.6%, -0.1%)
16 How Supplied/storage And Handling
XARELTO ® (rivaroxaban) Tablets are available in the strengths and packages uled below:
- 2.5 mg tablets are round, light yellow, and film-coated with a triangle pointing down above a "2.5" marked on one side and "Xa" on the other side. The tablets are supplied in the packages uled:
NDC 50458-577-60 Bottle containing 60 tablets NDC 50458-577-18 Bottle containing 180 tablets NDC 50458-577-10 Buler package containing 100 tablets (10 buler cards containing 10 tablets each) - 10 mg tablets are round, light red, biconvex film-coated tablets marked with a triangle pointing down above a "10" on one side, and "Xa" on the other side. The tablets are supplied in the packages uled:
NDC 50458-580-30 Bottle containing 30 tablets NDC 50458-580-90 Bottle containing 90 tablets NDC 50458-580-10 Buler package containing 100 tablets (10 buler cards containing 10 tablets each) - 15 mg tablets are round, red, biconvex film-coated tablets with a triangle pointing down above a "15" marked on one side and "Xa" on the other side. The tablets are supplied in the packages uled:
NDC 50458-578-30 Bottle containing 30 tablets NDC 50458-578-90 Bottle containing 90 tablets NDC 50458-578-10 Buler package containing 100 tablets (10 buler cards containing 10 tablets each) - 20 mg tablets are triangle-shaped, dark red film-coated tablets with a triangle pointing down above a "20" marked on one side and "Xa" on the other side. The tablets are supplied in the packages uled:
NDC 50458-579-30 Bottle containing 30 tablets NDC 50458-579-90 Bottle containing 90 tablets NDC 50458-579-89 Bulk bottle containing 1000 tablets NDC 50458-579-10 Buler package containing 100 tablets (10 buler cards containing 10 tablets each) - Starter Pack for treatment of deep vein thrombosis and treatment of pulmonary embolism:
NDC 50458-584-51 30-day starter buler pack containing 51 tablets: 42 tablets of 15 mg and 9 tablets of 20 mg
XARELTO ® (rivaroxaban) for oral suspension is available in the strength and package uled below:
NDC 50458-575-01 Supplied as white to off-white granules in an amber glass bottle containing 155 mg rivaroxaban packaged with two oral dosing syringes. After reconstitution with 150 mL of purified water, 1 mL of the suspension contains 1 mg rivaroxaban. STORAGE AND HANDLING SECTION
Discard reconstituted suspension after "Discard after" date written on the bottle.
Storage of tablets, granules and reconstituted suspension:
Store at room temperature between 20°C to 25°C (68°F to 77°F); excursions permitted between 15°C to 30°C (59°F to 86°F) [see USP Controlled Room Temperature].
Do not freeze the granules or reconstituted suspension.
Keep out of the reach of children.
17 Patient Counseling Information
For the tablets, advise the patient and/or caregiver to read the FDA-approved patient labeling (Medication Guide).
For the suspension, advise the patient and/or caregiver to read the FDA-approved patient labeling (Medication Guide and Instructions for Use).
Instructions for Patient Use
- Advise patients to take XARELTO only as directed.
- Remind patients to not discontinue XARELTO without first talking to their healthcare professional.
Adults
- Advise patients with atrial fibrillation to take XARELTO once daily with the evening meal.
- Advise patients for initial treatment of DVT and/or PE to take XARELTO 15 mg or 20 mg tablets with food at approximately the same time every day [see Dosage and Administration (2.1)] .
- Advise patients who are at a continued risk of recurrent DVT and/or PE after at least 6 months of initial treatment, to take XARELTO 10 mg once daily with or without food [see Dosage and Administration (2.1)].
- Advise patients who cannot swallow the tablet whole to crush XARELTO and combine with a small amount of applesauce followed by food [see Dosage and Administration (2.6)] .
- For patients requiring an NG tube or gastric feeding tube, instruct the patient or caregiver to crush the XARELTO tablet and mix it with a small amount of water before administering via the tube [see Dosage and Administration (2.6)] .
- If a dose is missed, advise the patient according to the instructions in the Full Prescribing Information based on their dosing schedule [see Dosage and Administration (2.5)] .
Pediatric Patients
- The adult caregiver should administer the dose. Advise caregivers to use the syringes provided in the original carton.
- Advise the caregiver whether the dose needs to be taken with food or not [see Dosage and Administration (2.2)] .
- Advise the caregiver the tablet must not be split in an attempt to provide a fraction of a tablet dose [see Dosage and Administration (2.2)] .
- If a child vomits or spits up the dose within 30 minutes after receiving the dose, a new dose should be given. However, if the child vomits more than 30 minutes after the dose is taken, the dose should not be re-administered and the next dose should be taken as scheduled. If a child vomits or spits up the dose repeatedly, the caregiver should contact the child's doctor right away [see Dosage and Administration (2.2)] .
- For children who are unable to swallow whole tablets, XARELTO oral suspension may be used.
- If a dose is missed, advise the patient according to the instructions in the Full Prescribing Information based on their dosing schedule [see Dosage and Administration (2.5)] .
Bleeding Risks
- Advise patients to report any unusual bleeding or bruising to their physician. Inform patients that it might take them longer than usual to stop bleeding, and that they may bruise and/or bleed more easily when they are treated with XARELTO [see Warnings and Precautions (5.2)] .
- If patients have had neuraxial anesthesia or spinal puncture, and particularly, if they are taking concomitant NSAIDs or platelet inhibitors, advise patients to watch for signs and symptoms of spinal or epidural hematoma, such as back pain, tingling, numbness (especially in the lower limbs), muscle weakness, and stool or urine incontinence. If any of these symptoms occur, advise the patient to contact his or her physician immediately [see Boxed Warning] .
Invasive or Surgical Procedures
Instruct patients to inform their healthcare professional that they are taking XARELTO before any invasive procedure (including dental procedures) is scheduled.
Concomitant Medication and Herbals
Advise patients to inform their physicians and dentists if they are taking, or plan to take, any prescription or over-the-counter drugs or herbals, so their healthcare professionals can evaluate potential interactions [see Drug Interactions (7)] .
Pregnancy and Pregnancy-Related Hemorrhage
- Advise patients to inform their physician immediately if they become pregnant or intend to become pregnant during treatment with XARELTO [see Use in Specific Populations (8.1)] .
- Advise pregnant women receiving XARELTO to immediately report to their physician any bleeding or symptoms of blood loss [see Warnings and Precautions (5.7)] .
Lactation
Advise patients to discuss with their physician the benefits and risks of XARELTO for the mother and for the child if they are nursing or intend to nurse during anticoagulant treatment [see Use in Specific Populations (8.2)] .
Females and Males of Reproductive Potential
Advise patients who can become pregnant to discuss pregnancy planning with their physician [see Use in Specific Populations (8.3)] .
Manufactured for: Janssen Pharmaceuticals, Inc. Titusville, NJ 08560
Licensed from: Bayer HealthCare AG 51368 Leverkusen, Germany
For patent information: www.janssenpatents.com
© 2011–2021 Janssen Pharmaceutical Companies
Spl Medguide Section
MEDICATION GUIDE XARELTO ® (zah-REL-toe) (rivaroxaban) tablets  XARELTO ® (zah-REL-toe) (rivaroxaban) oral suspension   This Medication Guide has been approved by the U.S. Food and Drug Administration Revised: 02/2023  What is the most important information I should know about XARELTO? XARELTO may cause serious side effects, including:
- Increased risk of blood clots if you stop taking XARELTO. People with atrial fibrillation (a type of irregular heart beat) that is not caused by a heart valve problem (non-valvular) are at an increased risk of forming a blood clot in the heart, which can travel to the brain, causing a stroke, or to other parts of the body. XARELTO lowers your chance of having a stroke by helping to prevent clots from forming. If you stop taking XARELTO, you may have increased risk of forming a clot in your blood. Do not stop taking XARELTO without talking to the doctor who prescribes it for you. Stopping XARELTO increases your risk of having a stroke. If you have to stop taking XARELTO, your doctor may prescribe another blood thinner medicine to prevent a blood clot from forming.
- Increased risk of bleeding. XARELTO can cause bleeding which can be serious and may lead to death. This is because XARELTO is a blood thinner medicine (anticoagulant) that lowers blood clotting. During treatment with XARELTO you are likely to bruise more easily, and it may take longer for bleeding to stop. You may have a higher risk of bleeding if you take XARELTO and have certain other medical problems. You may have a higher risk of bleeding if you take XARELTO and take other medicines that increase your risk of bleeding, including:
Tell your doctor if you take any of these medicines. Ask your doctor or pharmacist if you are not sure if your medicine is one uled above. Call your doctor or get medical help right away if you or your child develop any of these signs or symptoms of bleeding:
- aspirin or aspirin containing products
- long-term (chronic) use of non-steroidal anti-inflammatory drugs (NSAIDs)
- warfarin sodium (Coumadin ®, Jantoven ®)
- any medicine that contains heparin
- clopidogrel (Plavix ®)
- selective serotonin reuptake inhibitors (SSRIs) or serotonin norepinephrine reuptake inhibitors (SNRIs)
- other medicines to prevent or treat blood clots
- unexpected bleeding or bleeding that lasts a long time, such as:
- nose bleeds that happen often
- unusual bleeding from the gums
- menstrual bleeding that is heavier than normal or vaginal bleeding
- bleeding that is severe or you cannot control
- red, pink or brown urine
- bright red or black stools (looks like tar)
- cough up blood or blood clots
- vomit blood or your vomit looks like "coffee grounds"
- headaches, feeling dizzy or weak
- pain, swelling, or new drainage at wound sites
- Spinal or epidural blood clots (hematoma). People who take a blood thinner medicine (anticoagulant) like XARELTO, and have medicine injected into their spinal and epidural area, or have a spinal puncture have a risk of forming a blood clot that can cause long-term or permanent loss of the ability to move (paralysis). Your risk of developing a spinal or epidural blood clot is higher if:
If you take XARELTO and receive spinal anesthesia or have a spinal puncture, your doctor should watch you closely for symptoms of spinal or epidural blood clots. Tell your doctor right away if you have:
- a thin tube called an epidural catheter is placed in your back to give you certain medicine
- you take NSAIDs or a medicine to prevent blood from clotting
- you have a history of difficult or repeated epidural or spinal punctures
- you have a history of problems with your spine or have had surgery on your spine
- back pain
- tingling
- numbness
- muscle weakness (especially in your legs and feet)
- loss of control of the bowels or bladder (incontinence)
XARELTO is not for use in people with artificial heart valves. XARELTO is not for use in people with antiphospholipid syndrome (APS), especially with positive triple antibody testing. What is XARELTO? XARELTO is a prescription medicine used to: XARELTO is used with low dose aspirin to:
- reduce the risk of stroke and blood clots in adults who have a medical condition called atrial fibrillation that is not caused by a heart valve problem. With atrial fibrillation, part of the heart does not beat the way it should. This can lead to the formation of blood clots, which can travel to the brain, causing a stroke, or to other parts of the body.
- treat blood clots in the veins of your legs (deep vein thrombosis or DVT) or lungs (pulmonary embolism or PE)
- reduce the risk of blood clots from happening again in adults who continue to be at risk for DVT or PE after receiving treatment for blood clots for at least 6 months.
- help prevent a blood clot in the legs and lungs of adults who have just had hip or knee replacement surgery.
- help prevent blood clots in certain adults hospitalized for an acute illness and after discharge who are at risk of getting blood clots because of the loss of or decreased ability to move around (mobility) and other risks for getting blood clots and who do not have a high risk of bleeding.
XARELTO is used in children to:
- reduce the risk of serious heart problems, heart attack and stroke in adults with coronary artery disease (a condition where the blood supply to the heart is reduced or blocked).
- reduce the risk of a sudden decrease in blood flow to the legs, major amputation, serious heart problems or stroke in adults with peripheral artery disease (a condition where the blood flow to the legs is reduced) and includes adults who have recently had a procedure to improve blood flow to the legs.
XARELTO was not studied and is not recommended in children less than 6 months of age who:
- treat blood clots or reduce the risk of blood clots from happening again in children from birth to less than 18 years, after receiving at least 5 days of treatment with injectable or intravenous medicines used to treat blood clots.
- help prevent blood clots in children 2 years and older with congenital heart disease after the Fontan procedure.
- were less than 37 weeks of growth (gestation) at birth
- had less than 10 days of oral feeding, or
- had a body weight of less than 5.7 pounds (2.6 kg)
Do not take XARELTO if you or your child:
- currently have certain types of abnormal bleeding. Talk to your doctor before taking XARELTO if you currently have unusual bleeding.
- are allergic to rivaroxaban or any of the ingredients in XARELTO. See the end of this Medication Guide for a complete ul of ingredients in XARELTO.
Before taking XARELTO, tell your doctor about all of your medical conditions, including if you or your child: Tell all of your doctors and dentists that you or your child are taking XARELTO. They should talk to the doctor who prescribed XARELTO for you before you have any surgery, medical or dental procedure. Tell your doctor about all the medicines you or your child take, including prescription and over-the-counter medicines, vitamins, and herbal supplements. Some of your other medicines may affect the way XARELTO works, causing side effects. Certain medicines may increase your risk of bleeding. See " What is the most important information I should know about XARELTO?" Especially tell your doctor if you or your child take:
- have or ever had bleeding problems
- have liver or kidney problems
- have antiphospholipid syndrome (APS)
- are pregnant or plan to become pregnant. It is not known if XARELTO will harm your unborn baby.
- Tell your doctor right away if you become pregnant during treatment with XARELTO. Taking XARELTO while you are pregnant may increase the risk of bleeding in you or in your unborn baby.
- Females who are able to become pregnant: Talk with your doctor about pregnancy planning during treatment with XARELTO. Talk with your doctor about your risk for severe uterine bleeding if you are treated with blood thinner medicines, including XARELTO.
- If you take XARELTO during pregnancy tell your doctor right away if you have any signs or symptoms of bleeding or blood loss. See " What is the most important information I should know about XARELTO?" for signs and symptoms of bleeding.
- are breastfeeding or plan to breastfeed. XARELTO can pass into your breast milk. Talk to your doctor about the best way to feed your baby during treatment with XARELTO.
- ketoconazole
- erythromycin
- phenytoin
- St. John's wort
- ritonavir
- carbamazepine
- rifampin
How should I take XARELTO? If you take XARELTO for:
- Take XARELTO exactly as prescribed by your doctor.
- Do not change your dose or stop taking XARELTO unless your doctor tells you to. Your doctor may change your dose if needed.
- Your doctor will decide how long you should take XARELTO.
- XARELTO may need to be stopped for one or more days before any surgery or medical or dental procedure. Your doctor will tell you when to stop taking XARELTO and when to start taking XARELTO again after your surgery or procedure.
- If you need to stop taking XARELTO for any reason, talk to the doctor who prescribed XARELTO to you to find out when you should stop taking it. Do not stop taking XARELTO without first talking to the doctor who prescribes it to you.
- If you have difficulty swallowing XARELTO tablets whole, talk to your doctor about other ways to take XARELTO.
- Do not run out of XARELTO. Refill your prescription of XARELTO before you run out. When leaving the hospital following a hip or knee replacement, be sure that you will have XARELTO available to avoid missing any doses.
- If you take too much XARELTO, go to the nearest hospital emergency room or call your doctor right away.
For children who take XARELTO:
- Atrial fibrillation that is not caused by a heart valve problem:
- Take XARELTO 1 time a day with your evening meal.
- If you miss a dose of XARELTO, take it as soon as you remember on the same day. Take your next dose at your regularly scheduled time.
- Blood clots in the veins of your legs or lungs:
- Take XARELTO 1 or 2 times a day as prescribed by your doctor.
- For the 10 mg dose, take XARELTO with or without food.
- For the 15 mg and 20 mg doses, take XARELTO with food at the same time each day.
- If you miss a dose:
- If you take the 15 mg dose of XARELTO 2 times a day (a total of 30 mg of XARELTO in 1 day): Take XARELTO as soon as you remember on the same day. You may take 2 doses at the same time to make up for the missed dose. Take your next dose at your regularly scheduled time.
- If you take XARELTO 1 time a day: Take XARELTO as soon as you remember on the same day. Take your next dose at your regularly scheduled time.
- Hip or knee replacement surgery:
- Take XARELTO 1 time a day with or without food.
- If you miss a dose of XARELTO, take it as soon as you remember on the same day. Take your next dose at your regularly scheduled time.
- Blood clots in people hospitalized for an acute illness:
- Take XARELTO 1 time a day, with or without food, while you are in the hospital and after you are discharged as prescribed by your doctor.
- If you miss a dose of XARELTO, take it as soon as you remember on the same day. Take your next dose at your regularly scheduled time.
- Reducing the risk of serious heart problems, heart attack and stroke in coronary artery disease:
- Take XARELTO 2.5 mg 2 times a day with or without food.
- If you miss a dose of XARELTO, take your next dose at your regularly scheduled time.
- Take aspirin 75 to 100 mg once daily as instructed by your doctor.
- Reducing the risk of a sudden decrease in blood flow to the legs, major amputation, serious heart problems or stroke in people with peripheral artery disease including those who have recently had a procedure to improve blood flow to the legs:
- Take XARELTO 2.5 mg 2 times a day with or without food.
- If you miss a dose of XARELTO, take your next dose at your regularly scheduled time.
- Take aspirin 75 mg to 100 mg 1 time a day as instructed by your doctor.
- The dose of XARELTO depends on your child's body weight and will be calculated by your child's doctor. Your child's doctor will tell you if XARELTO can be given to your child with or without food.
- The adult caregiver should give the dose.
- If your child is taking the tablet, the tablet should be taken whole and should not be split in an attempt to provide a lower dose of XARELTO.
- If your child is taking the oral suspension, use the syringes provided in the original carton. The suspension will be prepared by the pharmacy. See the Instructions for Use included in the carton on how to properly give a dose of XARELTO oral suspension to your child.
- Do not switch between the XARELTO oral suspension or tablet without first talking to your doctor.
- If your child vomits or spits up:
- right after or within 30 minutes of taking the oral suspension, give a new full dose.
- more than 30 minutes after taking the oral suspension, do not give the dose again. Give the next dose at the regularly scheduled time.
- if vomiting or spitting up persists, contact your child's doctor right away.
- If your child misses a dose:
- If your child is taking XARELTO 1 time a day, give the dose as soon as you remember on the same day. If this is not possible, skip this dose and give the next dose at the regularly scheduled time.
- If your child is taking XARELTO 2 times a day, give the missed morning dose as soon as you remember. You may give the missed morning dose together with the evening dose. However, a missed evening dose can only be taken in the same evening.
- If your child is taking XARELTO 3 times a day, skip the missed dose and give the next dose at the regularly scheduled time.
What are the possible side effects of XARELTO? XARELTO may cause serious side effects: The most common side effect of XARELTO in adults was bleeding. The most common side effects of XARELTO in children include:
- bleeding
- vomiting
- cough
- inflamed stomach and gut
Call your doctor for medical advice about side effects. You may report side effects to FDA at 1 800-FDA-1088. How should I store XARELTO? Keep XARELTO and all medicines out of the reach of children. Discard XARELTO suspension after "Discard after" date written on the bottle.
- Store XARELTO tablets and suspension at room temperature between 68°F to 77°F (20°C to 25°C).
- Store syringes and bottle upright in the original carton for XARELTO suspension.
- Do not freeze XARELTO suspension.
General information about the safe and effective use of XARELTO. Medicines are sometimes prescribed for purposes other than those uled in a Medication Guide. Do not use XARELTO for a condition for which it was not prescribed. Do not give XARELTO to other people, even if they have the same symptoms that you have. It may harm them. You can ask your pharmacist or doctor for information about XARELTO that is written for health professionals. What are the ingredients in XARELTO? Active ingredient: rivaroxaban Inactive ingredients tablets: croscarmellose sodium, hypromellose, lactose monohydrate, magnesium stearate, microcrystalline cellulose, and sodium lauryl sulfate. The proprietary film coating mixture for XARELTO 2.5 mg tablets is Opadry ® Light Yellow and contains: ferric oxide yellow, hypromellose, polyethylene glycol 3350, and titanium dioxide. The proprietary film coating mixture for XARELTO 10 mg tablets is Opadry ® Pink and contains: ferric oxide red, hypromellose, polyethylene glycol 3350, and titanium dioxide. The proprietary film coating mixture for XARELTO 15 mg tablets is Opadry ® Red and contains: ferric oxide red, hypromellose, polyethylene glycol 3350, and titanium dioxide. The proprietary film coating mixture for XARELTO 20 mg tablets is Opadry ® II Dark Red and contains: ferric oxide red, polyethylene glycol 3350, polyvinyl alcohol (partially hydrolyzed), talc, and titanium dioxide. Inactive ingredients for oral suspension: anhydrous citric acid, hypromellose, mannitol, microcrystalline cellulose and carboxymethylcellulose sodium, sodium benzoate, sucralose, sweet and creamy flavor, and xanthan gum. Manufactured for: Janssen Pharmaceuticals, Inc. Titusville, NJ 08560 Licensed from: Bayer HealthCare AG 51368 Leverkusen, Germany For patent information: www.janssenpatents.com © 2011–2021 Janssen Pharmaceutical Companies Trademarks are property of their respective owners. For more information go to www.XARELTO-US.com or call 1-800-526-7736.
Instructions For Use Xarelto (zah-rel-toe) (rivaroxaban) For Oral Suspension

This Instructions for Use contains information on how to give a dose of XARELTO oral suspension.
Read this Instructions for Use before giving XARELTO and each time you get a refill. There may be new information. This leaflet does not take the place of talking with your doctor about your child's medical condition or treatment.
Important information:
- XARELTO suspension is for oral use only.
- Give XARELTO to your child exactly as prescribed by your doctor. The adult caregiver should give the dose. If you have questions, contact your doctor or pharmacist for more information on giving a dose.
- Only use the oral dosing syringe provided with XARELTO oral suspension. Contact your doctor or pharmacist if the oral dosing syringe is missing, lost or damaged.
Storage information
Store XARELTO oral suspension at room temperature between 68°F to 77°F (20°C to 25°C). Do not freeze.
Store the bottle upright with the oral dosing syringes in the original carton.
Keep XARELTO and all medicines out of reach of children.
XARELTO Oral Dosing Syringe:
Side 1: Dosing in milliliters (mL) Side 2: Dosing with color band The color band is an aid to withdraw the prescribed dose. (mL)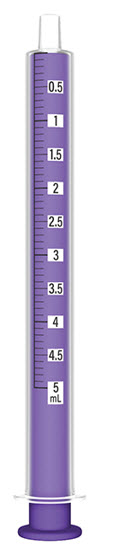
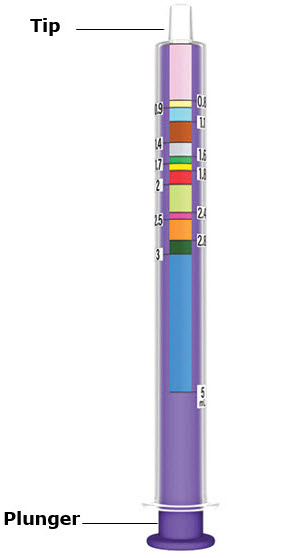
XARELTO Bottle
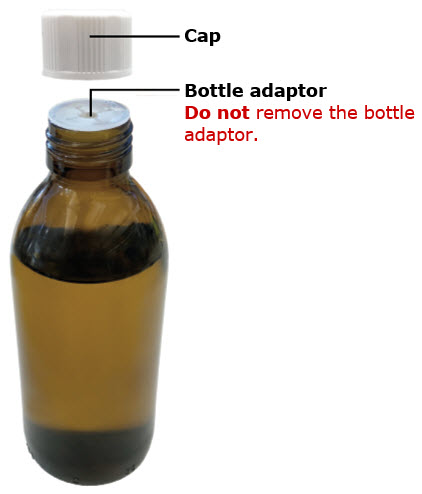
Step 1 Get ready
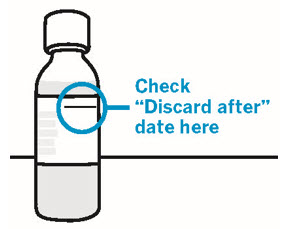
Check "Discard after" date on the XARELTO bottle.
If "Discard after" date has passed, do not use and call your doctor or pharmacist.

Wash hands.
Wash your hands well with soap and warm water.
Step 2 Prepare XARELTO

Shake bottle slowly for 10 seconds before each use.
Do not shake the bottle too fast to avoid foaming. Foaming may lead to giving the wrong dose.
Check XARELTO oral suspension.
If there are lumps or granules at the bottom of the bottle, shake the bottle slowly again for 10 seconds.
Step 3 Check the prescribed dose
Find your dose line.
You can use either side of the syringe to set your dose.
If using mL side of syringe:
Top of the plunger should line up with the prescribed mL.
If using color side of syringe:
Top of the plunger should line up with the prescribed mL dose line at the bottom of the color band.
Only use the oral dosing syringe provided with XARELTO oral suspension.
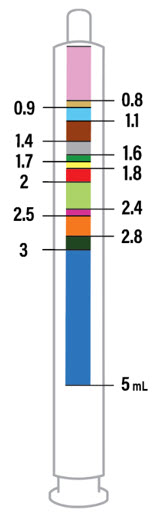
If your dose is more than 5 mL.
You will need to use the same syringe more than one time. Repeat Steps 4 and 5 to complete your dose. Ask your pharmacist if you are not sure.
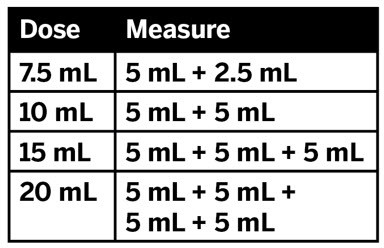
Step 4 Set prescribed dose
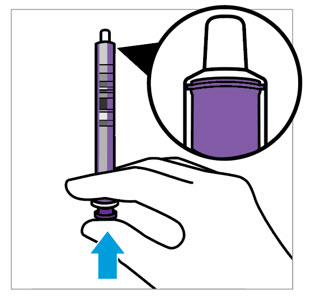
Push plunger all the way in to remove air.
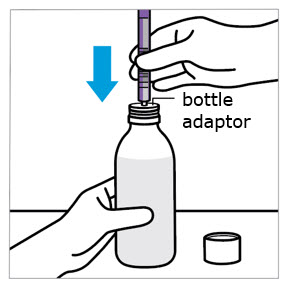
Insert oral dosing syringe into bottle adaptor.
Twist off the cap from the bottle.
Do not remove the bottle adaptor from the bottle.
Insert the syringe tip into the bottle adaptor.
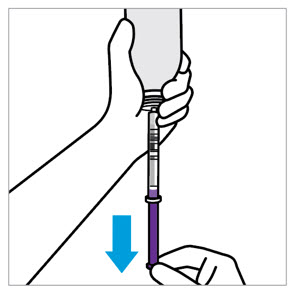
Fill oral dosing syringe.
Turn the bottle upside down, as shown.
Pull the plunger to fill the oral dosing syringe slightly past your prescribed dose line to help remove any air bubbles.
CAUTION:
Make sure you have enough medicine for a full dose. Do not take a partial dose.
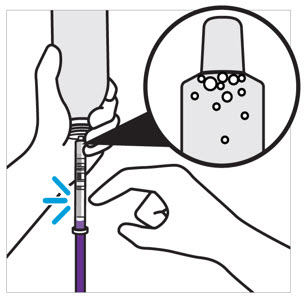
Tap syringe to move air bubbles to the top.
Doing this helps set the correct dose.
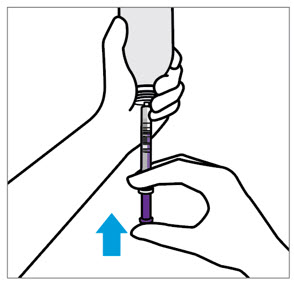
Adjust to your prescribed dose.
If using mL side of syringe: Push plunger to align with the prescribed dose line.
If using color side of syringe: Push plunger to align with the prescribed mL dose line at the bottom of the color band.
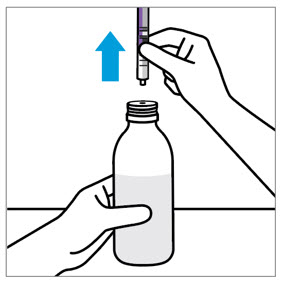
Remove oral dosing syringe.
Place the bottle on a flat surface.
Remove the oral dosing syringe from the bottle.
Step 5 Give the dose

Give the dose.
Place the oral dosing syringe gently into the child's mouth with the tip of the syringe pointing toward the cheek and slowly press the plunger.
This allows the child to swallow naturally.
Make sure the child swallows the full dose.
If your child vomits or spits out the medicine repeatedly, contact your child's doctor right away.
If your dose is more than 5 mL, you will need to use the same syringe more than one time. Repeat Steps 4 and 5 to complete your dose.
Step 6 Rinse and store
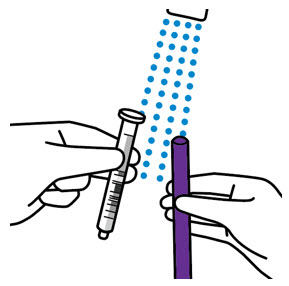
Close XARELTO bottle and rinse oral dosing syringe.
Rinse the oral dosing syringe with tap water and let it air dry.
Do not place the oral dosing syringe in the dishwasher.
Disposing XARELTO bottle and syringe
- Throw the XARELTO bottle away in your household trash.
- Throw away any used oral dosing syringe with the opening of a new XARELTO bottle.
- Do not pour XARELTO suspension down the drain (for example: sink, toilet, shower or tub).
- Do not recycle the bottle.
Manufactured for: Janssen Pharmaceuticals, Inc. Titusville, NJ 08560 Licensed from: Bayer HealthCare AG 51368 Leverkusen, Germany
For patent information: www.janssenpatents.com
© 2021 Janssen Pharmaceutical Companies
This Instructions for Use has been approved by the U.S. Food and Drug Administration. Issued: 02/2023
Principal Display Panel - 2.5 Mg Tablet Bottle Label
NDC 50458-577-60
Xarelto ® (rivaroxaban) Tablets 2.5 mg
Dispense the accompanying Medication Guide to each patient.
Each tablet contains 2.5 mg of rivaroxaban.
Rx only
60 Tablets

Principal Display Panel - 10 Mg Tablet Bottle Label
NDC 50458-580-30
Xarelto ® (rivaroxaban) Tablets 10 mg
Dispense the accompanying Medication Guide to each patient.
Each tablet contains 10 mg of rivaroxaban.
Rx only
30 Tablets

Principal Display Panel - 15 Mg Tablet Bottle Label
NDC 50458-578-30
Xarelto ® (rivaroxaban) Tablets 15 mg
Dispense the accompanying Medication Guide to each patient.
Each tablet contains 15 mg of rivaroxaban.
Rx only
30 Tablets

Principal Display Panel - 20 Mg Tablet Bottle Label
NDC 50458-579-30
Xarelto ® (rivaroxaban) Tablets 20 mg
Dispense the accompanying Medication Guide to each patient.
Each tablet contains 20 mg of rivaroxaban.
Rx only
30 Tablets

Principal Display Panel - Kit Carton
Xarelto ® (rivaroxaban) Tablets
NDC 50458-584-51 Rx only
Please see full Prescribing Information, including BOXED WARNINGS, and Medication Guide inside.
Starter Pack for treatment of deep vein thrombosis and treatment of pulmonary embolism
Days 1-21 15mg per tablet, twice daily 42 tablets
Days 22-30 20mg per tablet, once daily 9 tablets
First 30-day supply
LIFT HERE TO OPEN
Principal Display Panel - 1 Mg/ml Bottle Carton
NDC 50458-575-01
Xarelto ® (rivaroxaban) for Oral Suspension
1 mg/mL (when reconstituted)
Pharmacist:
- Must reconstitute before dispensing.
- Counsel caregiver on proper use.
ATTENTION: Dispense the enclosed Medication Guide to each patient.
For Oral Use Only
Rx only janssen

DISCLAIMER:
"This tool does not provide medical advice, and is for informational and educational purposes only, and is not a substitute for professional medical advice, treatment or diagnosis. Call your doctor to receive medical advice. If you think you may have a medical emergency, please dial 911."
"Do not rely on openFDA to make decisions regarding medical care. While we make every effort to ensure that data is accurate, you should assume all results are unvalidated. We may limit or otherwise restrict your access to the API in line with our Terms of Service."
"This product uses publicly available data from the U.S. National Library of Medicine (NLM), National Institutes of Health, Department of Health and Human Services; NLM is not responsible for the product and does not endorse or recommend this or any other product."
PillSync may earn a commission via links on our site
